

Summary Card
Overview
The nose is a complex, layered structure composed of skin, muscles, bones, and cartilage, with key external landmarks guiding clinical assessment and anthropometric measurements for surgical planning.
Landmarks and Measurements
Key nasal landmarks guide rhinoplasty planning; ideal angles include a nasofrontal angle of 115-130° and a nasolabial angle of 90-105°, with tip projection and length assessed via Goode’s ratio and facial thirds.
Skin and Soft Tissue Envelope
The nasal skin-soft tissue envelope includes key layers: Skin, superficial and deep fat, nasal SMAS, and periosteum/perichondrium. Muscles are functionally grouped into four categories.
The Bony Vault
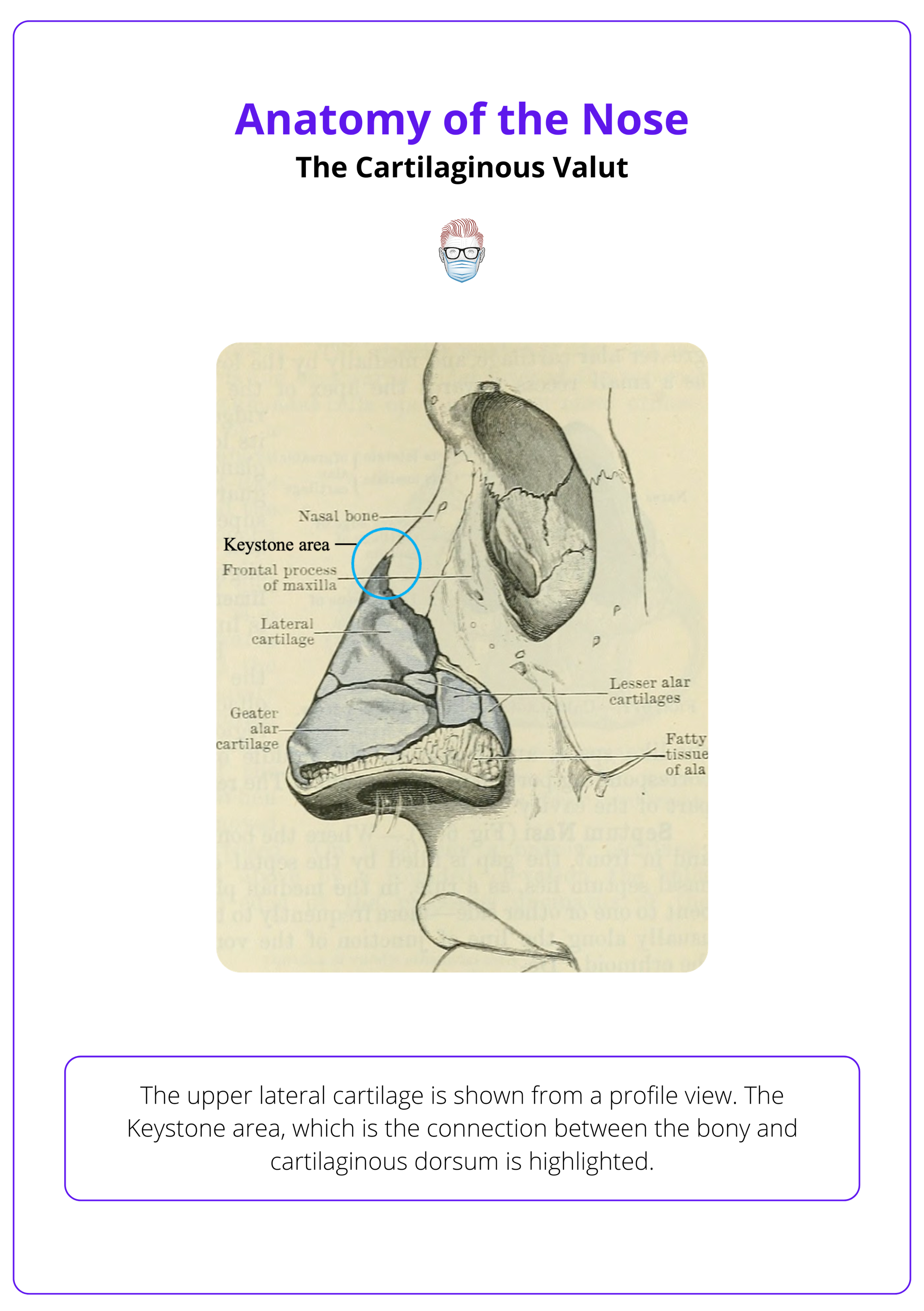
The bony vault, formed by nasal bones and maxilla, connects with frontal and ethmoid bones; the keystone area which is crucial for dorsal support, is the bone-cartilage overlap on the dorsum.
The Cartilaginous Vault
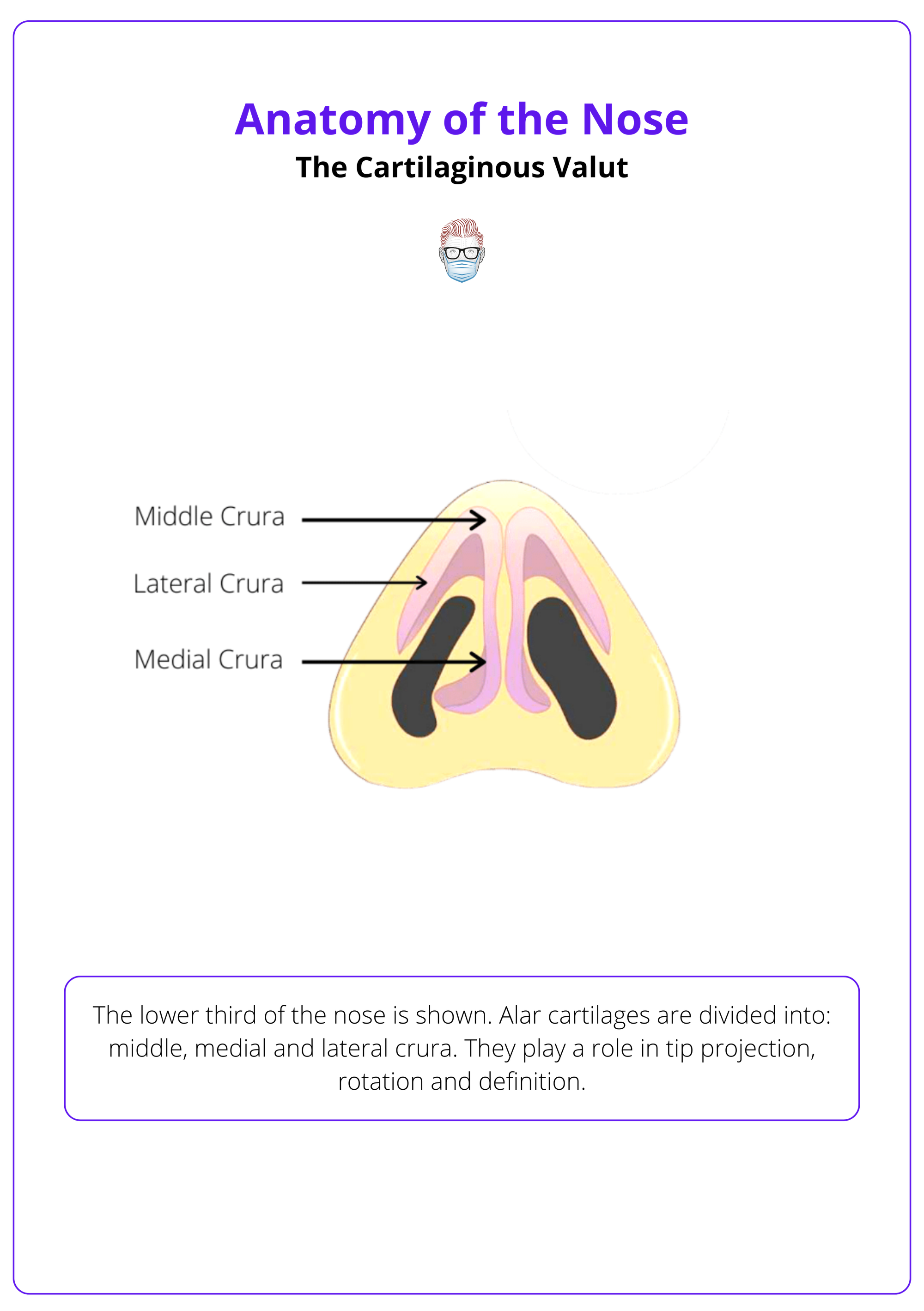
The middle third includes ULCs and dorsal septum, forming dorsum and the internal valve. The lower third has LLCs, accessory cartilages, and fibrofatty tissue, shaping tip, columella, and alae.
Internal Anatomy of the Nose
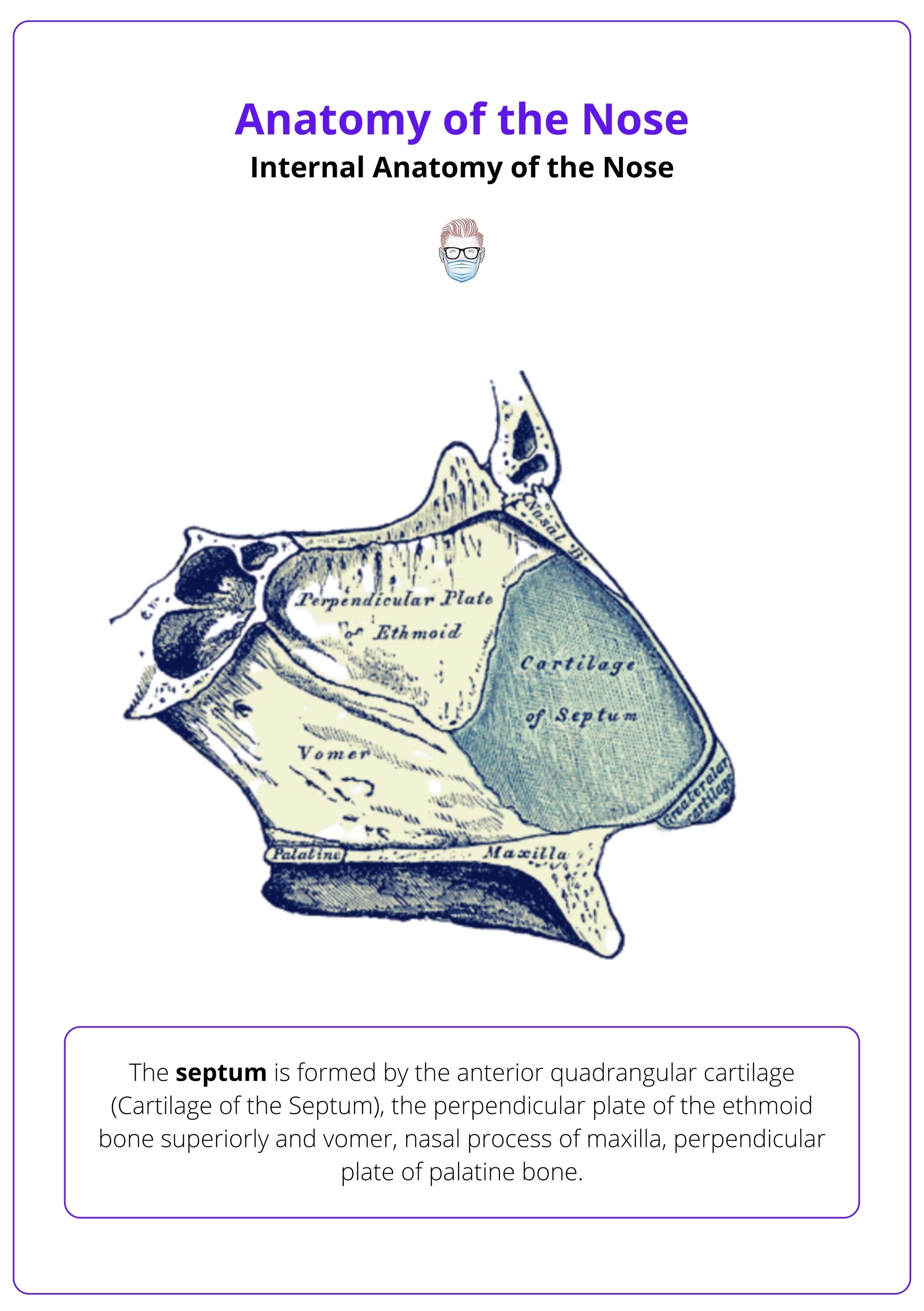
The internal nose consists of the septum, which divides the nasal cavity; the internal valve, formed between the ULCs and septum; and the turbinates, which filter and humidify inspired air.
Blood Supply
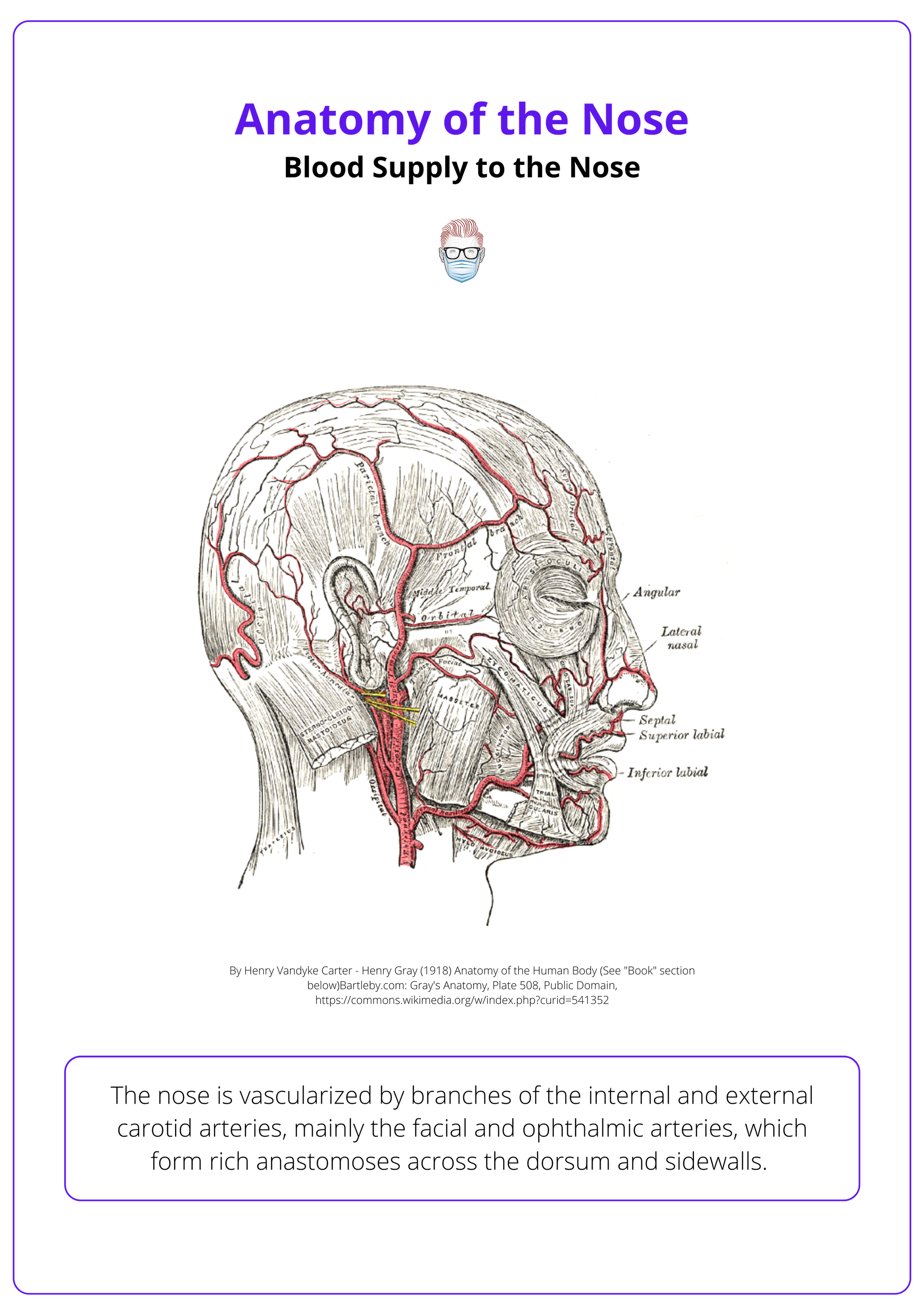
The nose is vascularized by branches of the internal and external carotid arteries, mainly the facial and ophthalmic arteries, which form rich anastomoses across the dorsum and sidewalls.
Nerve Supply
The external nose is innervated by the trigeminal nerve (CN V), with V1 supplying the cephalic regions and V2 the caudal lateral areas.
Updated by: Dr Benedetta Agnelli, Educational Fellow
Verified by thePlasticsFella ✅
Overview of Anatomy of the Nose
The nose is a complex, layered structure composed of skin, muscles, bones, and cartilage, with key external landmarks guiding clinical assessment and anthropometric measurements for surgical planning.
The nose serves both aesthetic and functional roles and is one of the most structurally and anatomically intricate regions of the face. It is composed of layered components, including skin, fat, soft tissue, muscles, cartilage, and bone. Each of these contributes to nasal form, symmetry, and airway function.
The nasal framework is broadly divided into,
- Upper Third (Bony Vault): Formed by paired nasal bones.
- Middle Third (Cartilaginous Vault): Shaped by the upper lateral cartilages and the septum.
- Lower Third (Tip Complex): Formed by the lower lateral cartilages and surrounding soft tissue.
From an external perspective, key surface landmarks such as the radix, dorsum, tip, and alar margins guide both aesthetic assessment and surgical planning. Internally, the nasal septum and turbinates regulate airflow, humidification, and filtration.
Landmarks and Measurements of the Nose
Key nasal landmarks guide rhinoplasty planning; ideal angles include a nasofrontal angle of 115-130° and a nasolabial angle of 90-105°, with tip projection and length assessed via Goode’s ratio and facial thirds.
External nasal anatomy provides a crucial reference for both aesthetic evaluation and surgical intervention. Surface landmarks not only reflect underlying anatomical structures but also help determine the proportion, symmetry, and balance of the nose relative to the rest of the face.
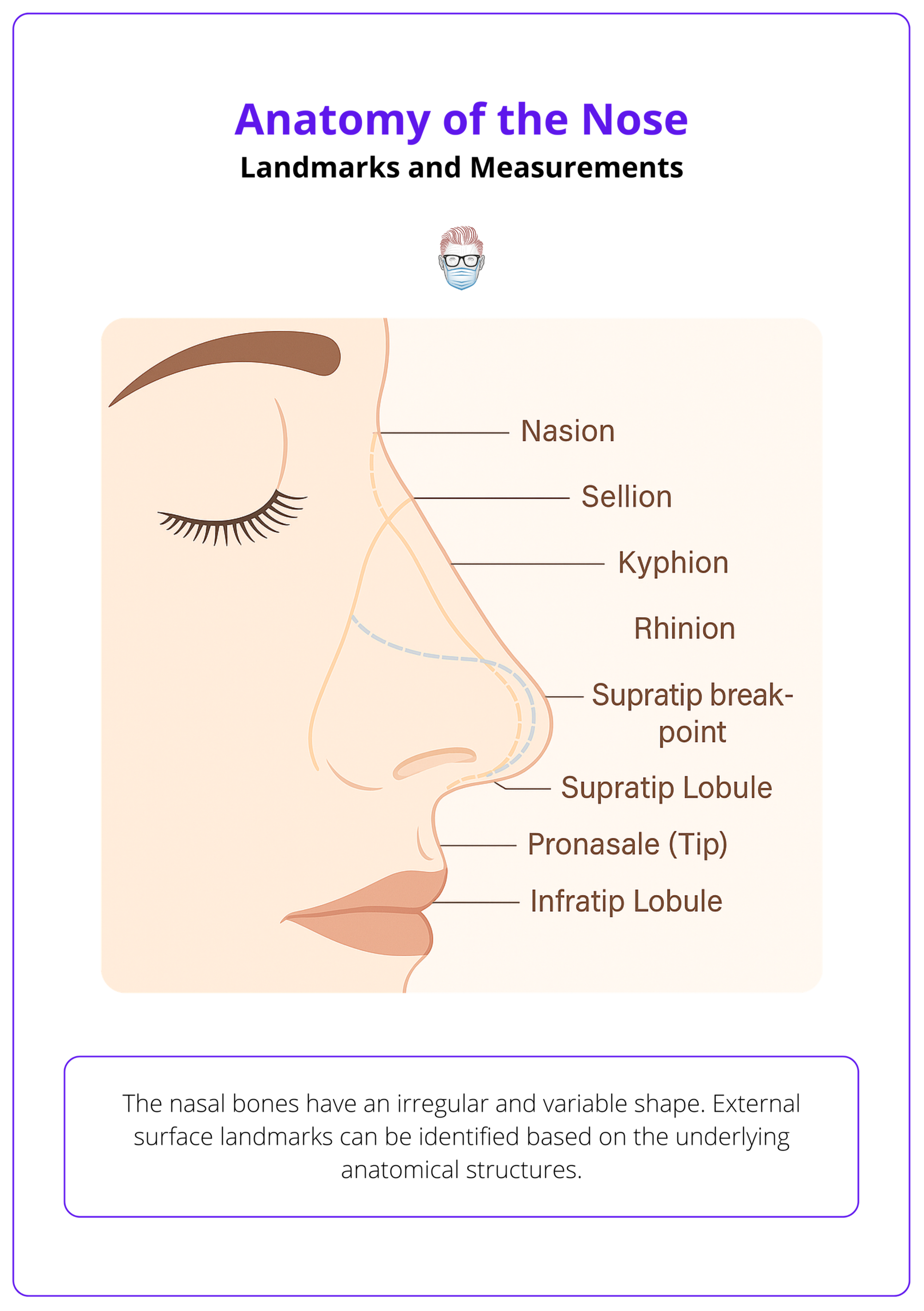
The nose is commonly divided into thirds, from cephalic to caudal: nasion, rhinion, and tip. Important anatomical landmarks include,
- Nasion (Radix region): Midpoint of the nasofrontal suture.
- Sellion: Deepest point of the nasofrontal angle; soft tissue correlate of the nasion.
- Kyphion: Most prominent point of the bony nasal dorsum.
- Rhinion: Caudal edge of the nasal bones, marking transition to cartilage.
- Pronasale (Tip): Most anterior projecting point of the nose.
- Supratip Breakpoint: Junction between dorsum and tip.
- Supratip Lobule: Region between pronasale and supratip breakpoint.
- Infratip Lobule: Area between the tip and nostril apex (columellar-lobular junction).
The image below illustrates external surface landmarks of the nose.
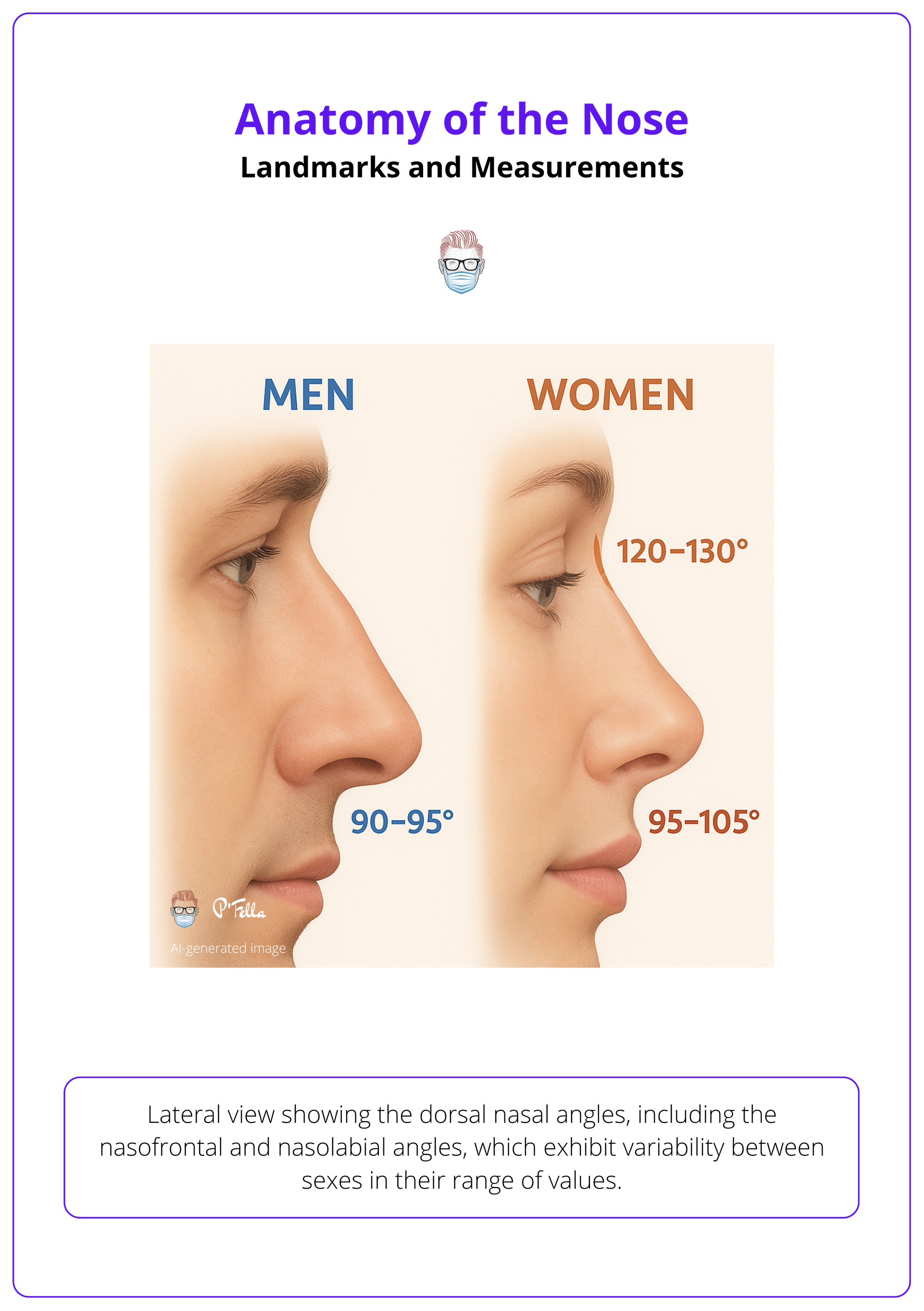
To achieve nasal-facial harmony, several anthropometric ideals are considered.
- Nasofrontal Angle: 115°–130°.
- Nasolabial Angle: ~90°–95° in men; 95°–105° in women.
- Tip Projection: Goode’s ratio = ~0.55–0.6 × nasal length.
- Nasal Length: Ideally, two-thirds of total facial length.
- Frontal View: Nose should fall within vertical lines from the medial canthi; alar base width should match intercanthal distance.
These measurements help guide surgical decision-making in rhinoplasty and contribute to achieving both functional and aesthetic goals.
Skin and Soft Tissue Envelope
The nasal skin – soft tissue envelope includes key layers: skin, superficial and deep fat, nasal SMAS, and periosteum/perichondrium. Muscles are functionally grouped into four categories.
The skin and soft tissue envelope (STE) of the nose determines how underlying structural changes manifest externally. Understanding its composition and variability is essential for surgical planning, especially in rhinoplasty, where skin thickness influences the predictability of outcomes.
Skin
Skin thickness is one of the most important factors to evaluate preoperatively. It directly affects the extent to which underlying structural changes will be visible externally.
- Upper Two-Thirds: Thinner, more mobile skin (Lessard, 1985).
- Lower Third: Thicker, more sebaceous (O'Neal, 1999).
The soft tissue layers between the skin and the osteocartilaginous skeleton are,
- Superficial fatty layer (panniculus adiposus).
- Fibromuscular layer (nasal SMAS - subcutaneous musculoaponeurotic system).
- Deep fatty layer.
- Periosteum or perichondrium.
The deep fatty layer is of particular surgical importance, as it contains the major superficial blood vessels and motor nerves. The ideal plane of surgical dissection lies just beneath this layer.
Muscle
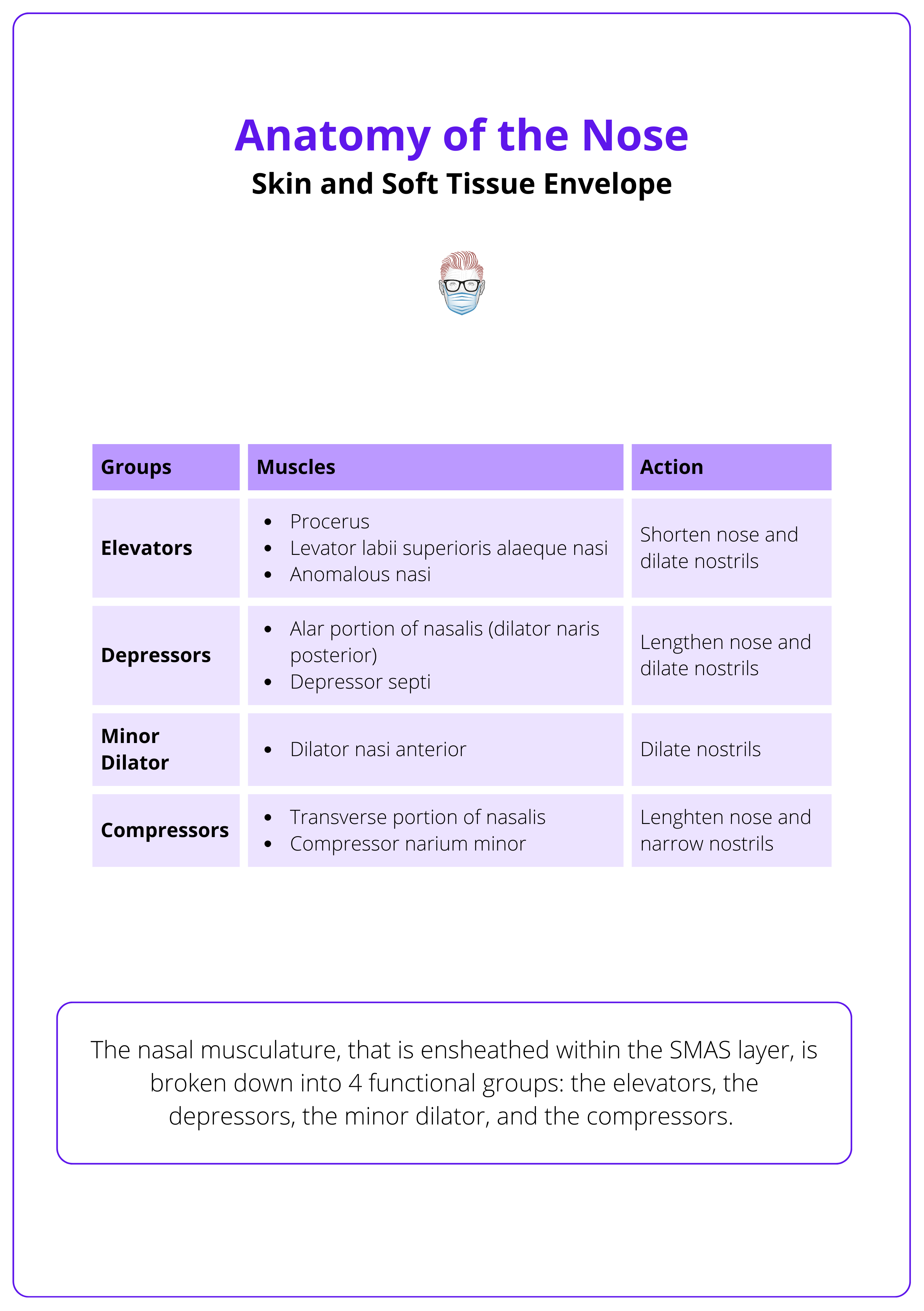
The nasal muscles are categorized into four functional groups (Griesman, 1944 & Letourneau, 1988).
- Elevator muscles (shorten the nose, dilate the nostrils).
- Procerus.
- Levator labii superioris alaeque nasi.
- Anomalous nasi.
- Depressor muscles (lengthen the nose, dilate the nostrils).
- Depressor septi.
- Alar part of the nasalis (dilator naris posterior).
- Compressor muscles (lengthen the nose, narrow the nostrils).
- Transverse portion of the nasalis.
- Compressor narium minor.
- Minor dilator muscle.
- Dilator naris anterior.
All nasal muscles are innervated by branches of the zygomaticotemporal division of the facial nerve.
The nasal musculature is summarised in the table below (Griesman, 1944).
Bony Vault of the Nose
The bony vault, formed by nasal bones and maxilla, connects with frontal and ethmoid bones; the keystone area, crucial for dorsal support, is the bone-cartilage overlap on the dorsum.
The upper third of the nose is the rigid bony framework that provides dorsal support and defines the nasal profile. Its integrity and shape are essential considerations in both functional and aesthetic rhinoplasty.
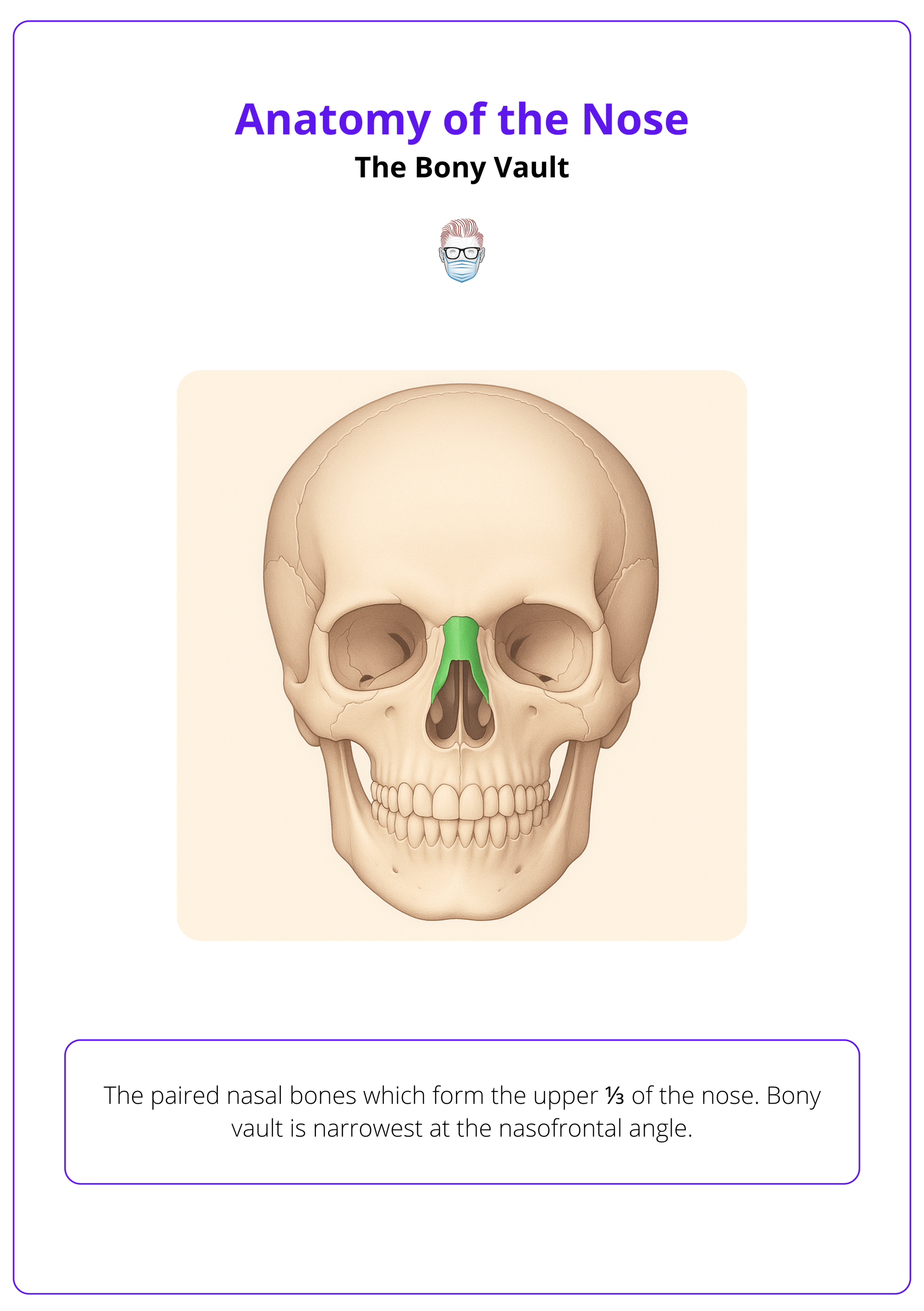
The bony vault represents the upper 1/3 of the nose which consists of,
- Paired nasal bones.
- Ascending (frontal) processes of the maxilla.
In relation to adjacent bones, the nasal bone interdigitates with,
- Superior: Nasal process of the frontal bone.
- Lateral: Frontal process of the maxilla.
- Posterior: Perpendicular plate of the ethmoid.
- Medial: Paired nasal bones at midline forming the roof of nasal cavity.
A crucial structural region, known as the keystone area, lies just caudal to the intercanthal line. It includes the overlap of four major elements,
- Nasal bones
- Upper lateral cartilages
- Cartilaginous septum
- Perpendicular plate of the ethmoid
This confluence provides essential support to the nasal dorsum and is a critical consideration in rhinoplasty.
The bony vault of the nose is illustrated below.
Cartilaginous Vault of the Nose
The middle third includes ULCs and dorsal septum, forming dorsum and internal valve. The lower third has LLCs, accessory cartilages, and fibrofatty tissue, shaping the tip, columella, and alae, supported by interdomal and dermocartilaginous ligaments.
The cartilaginous vault forms the structural and aesthetic core of the mid and lower nose. It contributes to dorsal contour, tip definition, and internal valve competence, and is composed of distinct but interrelated units.
The middle 1/3 of the nasal cavity is a cartilaginous structure which includes,
- Upper Lateral Cartilages (ULCs): Paired, connected medially to the dorsal septum and superiorly to the nasal bones. These define the upper cartilaginous dorsum and contribute to the internal valve angle. Laterally, the ULCs are unsupported by bone and held in place by soft tissue attachments.
- Dorsal Cartilaginous Septum (Quadrangular Cartilage): Central support structure of the nose, extending anteriorly from the perpendicular plate of the ethmoid.
- External Lateral Triangle: A mucosa-lined lateral recess that may contain sesamoid cartilages and impact nasal airflow.
These structures form a rigid yet flexible vault that contributes to the nasal dorsum and internal nasal valve.
The cartilaginous vault of the nose is illustrated below.
Preserving the mucoperichondrium between ULCs and septum is vital to maintain internal valve function during surgery.
The lower 1/3 of the nose comprises,
- Lower Lateral Cartilages (LLCs) are divided into,
- Medial Crura: Contribute to the columellar shape and projection.
- Middle (Intermediate) Crura: Domal and lobular segments, critical for tip definition.
- Lateral Crura: Support the alar rim and shape the nostril sidewalls.
- Accessory Cartilages: Small, often variable pieces between the LLCs and piriform aperture.
- Fibrofatty Tissue: Completes the contour of the nasal tip and nostrils.
Ligamentous Support
- Interdomal Ligament: Connects medial and middle crura anteriorly.
- Dermocartilaginous Ligament (Pitanguy Ligament): Vertical fibers anchoring the tip to the skin, contributing to tip stability and definition.
- Scroll Area: The junction between the lateral crura and ULCs.
Each component must be considered in tip rotation, projection, and support during rhinoplasty.
The lower 1/3 cartilaginous vault of the nose is illustrated below.
Internal Anatomy of the Nose
The internal nose consists of the septum, which divides the nasal cavity; the internal valve, formed between the ULCs and septum; and the turbinates, which filter and humidify inspired air.
A clear understanding of internal nasal anatomy is essential in rhinoplasty and septoplasty to preserve or restore nasal airflow. The internal structures contribute significantly to nasal function and must be carefully evaluated in both functional and aesthetic procedures.
Nasal Septum
The septum divides the nasal cavity and consists of,
- Cartilaginous Component: The quadrangular cartilage anteriorly.
- Bony Components: Perpendicular plate of the ethmoid superiorly, and the vomer inferiorly, articulating with the nasal crest of the maxilla and palatine bones.
The anterior nasal spine represents the caudal attachment of the septum.
Internal Nasal Valve
Formed by the junction of the upper lateral cartilages (ULCs) and the septum, the internal nasal valve is the narrowest segment of the nasal airway.
Its angle, normally between 10–15°, critically affects nasal airflow.
Turbinates
The superior, middle, and inferior turbinates are scroll-like bony structures lined with vascularized mucosa.
They humidify and filter inspired air and may become hypertrophic in response to septal deviations. The inferior turbinate, in particular, is frequently addressed in nasal surgeries to improve airflow and exposure.
Internal nose anatomy is illustrated below.
Blood Supply to the Nose
The nose is vascularized by branches of the internal and external carotid arteries, mainly the facial and ophthalmic arteries, which form rich anastomoses across the dorsum and sidewalls. Venous drainage mirrors arterial pathways via facial, pterygoid, and ophthalmic veins.
The nose receives a rich vascular supply from both the internal and external carotid arteries (Letourneau, 1988).
Arterial Supply
The nose receives blood from both the external and internal carotid systems.
- External Carotid System
- Facial artery gives rise to,
- Superior Labial Artery: Contributes columellar branches to the tip.
- Angular Artery: Supplies the sidewalls and dorsum.
- Facial artery gives rise to,
- Internal Carotid System
- Ophthalmic Artery (branch of internal carotid) gives off,
- Anterior Ethmoidal Artery
- Dorsal Nasal Artery
- External Nasal Branch
- Ophthalmic Artery (branch of internal carotid) gives off,
- The dorsal nasal artery anastomoses with the angular artery, forming a robust subdermal plexus across the dorsum.
These extensive anastomoses create a rich axial vascular network, essential for,
- Skin flap viability
- Healing post-rhinoplasty
- Avoiding ischemic complications
Venous Drainage
Venous return follows a path similar to the arterial system.
- Facial vein
- Pterygoid venous plexus
- Ophthalmic veins
Nerve Supply to the Nose
The external nose is innervated by branches of the trigeminal nerve (CN V), with V1 supplying the cephalic regions and V2 the caudal lateral areas.
The external nose receives its sensory innervation primarily from branches of the trigeminal nerve (CN V), specifically,
- Ophthalmic Nerve (V1): Radix, upper dorsum, and sidewalls of the nose (supratrochlear and infratrochlear nerves, branches of V1).
- Maxillary Nerve (V2): Infraorbital nerve, a branch of V2, supplies the lower lateral sidewalls of the nose, portions of the columella, and the lateral vestibule. This nerve is frequently targeted with an infraorbital nerve block in rhinoplasty procedures performed under local anesthesia.
Together, these branches provide a rich and overlapping sensory network.
The external nasal nerve, emerging at the keystone area, supplies the nasal tip and caudal dorsum, and it is often injured during rhinoplasty, causing temporary or persistent numbness.
Conclusion
1. Nasal Anatomy Overview: Understanding of the nose's complex structure, including its skin, muscles, bones, and cartilage, essential for clinical assessment and surgical planning.
2. Landmarks and Ideal Measurements: Learn about key nasal landmarks for rhinoplasty, including ideal angles and measurements, such as the nasofrontal angle, nasolabial angle, and Goode’s ratio for tip projection and length.
3. Skin and Soft Tissue Envelope: Review the layers of the nasal skin-soft tissue envelope, including the skin, fat, SMAS, and periosteum/perichondrium, along with the functional grouping of muscles.
4. The Bony Vault: Understanding the structure of the bony vault, including the nasal bones and maxilla, and the importance of the keystone area for dorsal support.
5. The Cartilaginous Vault: Understanding the cartilaginous components, including ULCs, LLCs, and fibrofatty tissue, and their role in shaping the tip, columella, and alae.
6. Internal Anatomy of the Nose: Identify the components of the internal nose, including the septum, internal valve, and turbinates, which are critical for airflow filtration and humidification.
7. Blood Supply to the Nose: Understand the vascularization of the nose, focusing on the arterial supply from the internal and external carotid arteries, along with venous drainage.
8. Nerve Supply to the Nose: Learn about the sensory innervation of the external nose, provided by the trigeminal nerve (CN V), with V1 innervating the cephalic regions and V2 the caudal lateral areas.
Further Reading
- Lessard M-L, Daniel RK. Surgical Anatomy of Septorhinoplasty. Archives of Otolaryngology – Head and Neck Surgery. Published online January 1, 1985:25-29. doi:10.1001/archotol.1985.00800030059006
- Oneal RM, Beil RJ Jr, Schlesinger J. SURGICAL ANATOMY OF THE NOSE. Otolaryngologic Clinics of North America. Published online February 1999:145-181. doi:10.1016/s0030-6665(05)70119-5
- Letourneau A, Daniel R. The superficial musculoaponeurotic system of the nose. Plast Reconstr Surg. 1988;82(1):48-57.
- Griesman B. Muscles And Cartilages Of The Nose From The Standpoint Of A Typical Rhinoplasty. Archives of Otolaryngology – Head and Neck Surgery. Published online April 1, 1944:334-341. doi:10.1001/archotol.1944.00680010348009
- Lazovic GD, Daniel RK, Janosevic LB, Kosanovic RM, Colic MM, Kosins AM. Rhinoplasty: the nasal bones - anatomy and analysis. Aesthet Surg J. 2015 Mar;35(3):255-63. doi: 10.1093/asj/sju050. PMID: 25805278.
- Fonseca E, Baldini N, Alomani M, Saban Y. Nasal Bones Anatomy and Analysis for Dorsal Preservation Rhinoplasty. Aesthet Surg J. 2023 Feb 21;43(3):NP227-NP228. doi: 10.1093/asj/sjac300. PMID: 36402140; PMCID: PMC9942437.
- Sowder JC, Thomas AJ, Ward PD. Essential Anatomy and Evaluation for Functional Rhinoplasty. Facial Plast Surg Clin North Am. 2017 May;25(2):141-160. doi: 10.1016/j.fsc.2016.12.001. PMID: 28340646.
- Lane AP. Nasal anatomy and physiology. Facial Plast Surg Clin North Am. 2004 Nov;12(4):387-95, v. doi: 10.1016/j.fsc.2004.04.001. PMID: 15337106.
