

Summary Card
Overview
Prominent ear (projection >2 cm or auriculocephalic angle >30°) is surgically corrected by otoplasty. The most common causes are antihelical fold deficiency and/or conchal hypertrophy.
Aetiology
Prominent ear deformities arise from a combination of congenital cartilage anomalies, neonatal molding factors, and potential genetic inheritance.
Auricular Anatomy
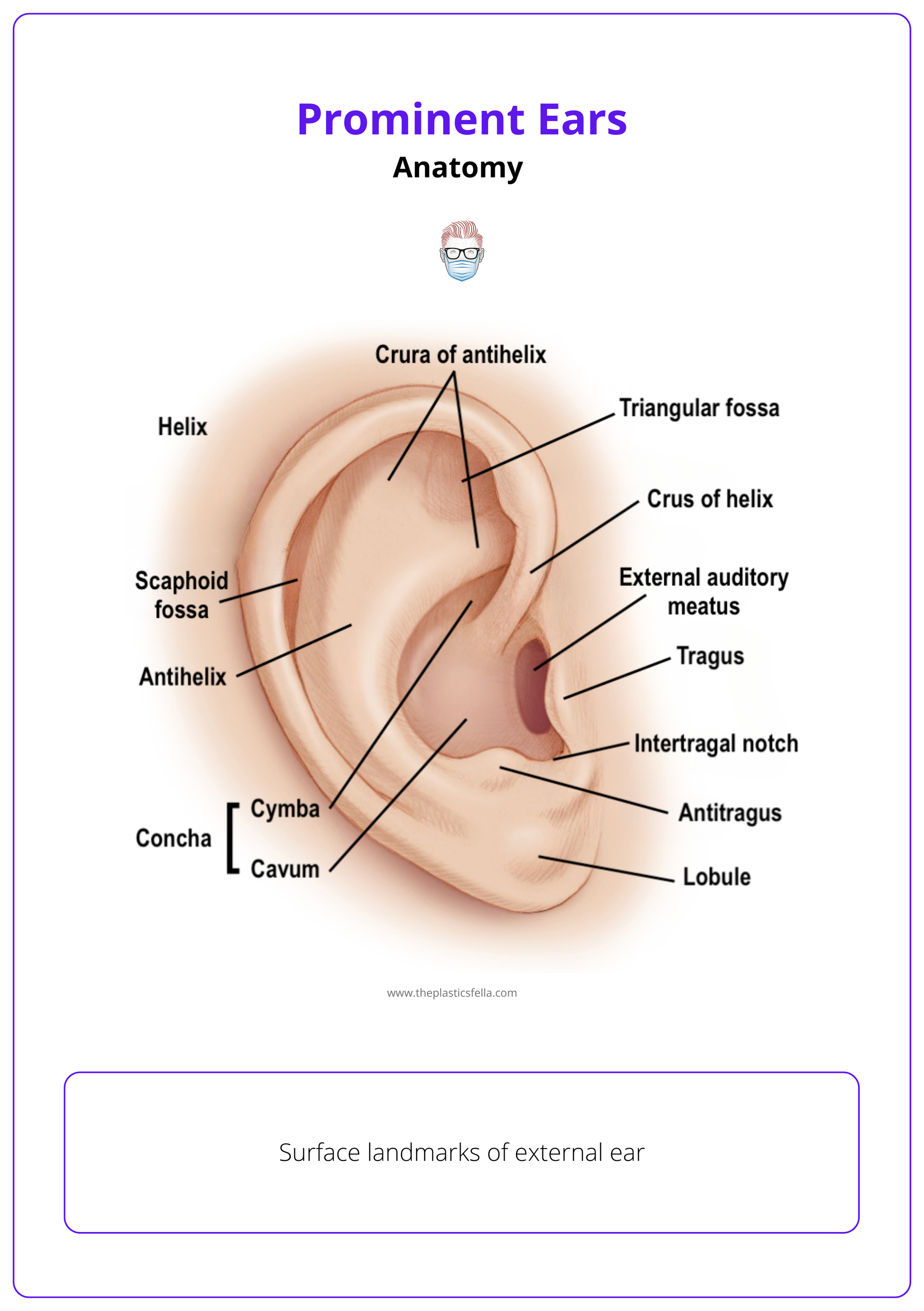
The auricle is divided into subunits: helix, antihelix, concha, and lobule. Accurate subunit identification is essential for tailored surgical correction.
Clinical Assessment
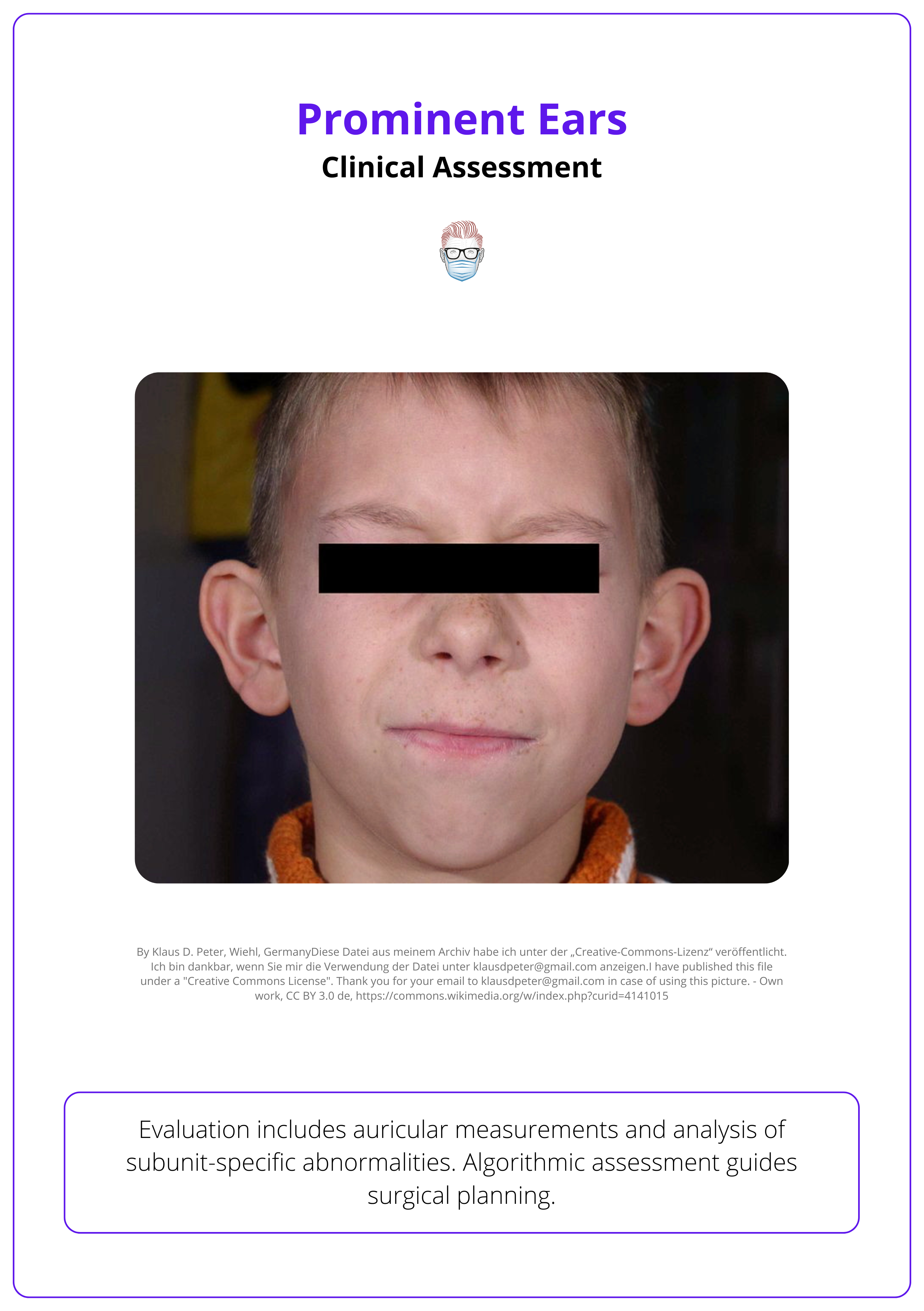
Evaluation includes auricular measurements and analysis of subunit-specific abnormalities. Algorithmic assessment guides surgical planning.
Decision Making
Effective correction of prominent ears relies on identifying the dominant anatomical deformity and selecting a tailored surgical technique.
Surgical Technique (Otoplasty)
Surgical correction of prominent ears relies on a subunit-based approach; tailoring techniques like Mustardè, Converse, Argamaso, and Furnas to specific auricular deformities for natural results.
Post-Operative Care & Complications
Postoperative otoplasty care includes short-term compression, soft headband use, antibiotics, activity restrictions, and monitoring for complications like hematoma and wound dehiscence.
Updated by: Dr Benedetta Agnelli, Educational Fellow
Verified by thePlasticsFella ✅
Overview of Prominent Ears
Prominent ear (ear projection >2 cm or auriculocephalic angle >30°) is surgically corrected by otoplasty. The most common causes are antihelical fold deficiency and/or conchal hypertrophy.
Prominent ears are characterized by an auriculocephalic angle exceeding 30° or an auricular projection greater than 2 cm from the mastoid surface.
Despite normal anatomical structures, these ears appear overly protruding due to specific morphological imbalances; most frequently, an underdeveloped antihelical fold and/or conchal hypertrophy.
The three key pathological features of this deformity are,
- Absent or underdeveloped antihelical fold.
- Conchal excess >1.5 cm.
- Conchoscaphal angle >90°.
Otoplasty refers to the surgical reshaping or repositioning of the auricle to correct these abnormalities.
Prominent ears affect approximately 5% of the population, making them the commonest congenital auricular deformity (Kelley, 2003). Often bilateral, can lead to psychosocial distress.
Aetiology of Prominent Ears
Prominent ear deformities arise from a combination of congenital cartilage anomalies, neonatal molding factors, and potential genetic inheritance.
The development of prominent ears involves both intrinsic cartilage anomalies and extrinsic molding influences.
- Congenital Cartilage Anomalies: The most common cause includes an underdeveloped antihelical fold or an enlarged conchal bowl.
- Perinatal Molding: External pressure during vaginal delivery or in utero can temporarily alter ear shape.
- Neonatal Cartilage Malleability: High estrogen levels in the first weeks of life make auricular cartilage soft and moldable.
- Familial Traits: An autosomal dominant inheritance pattern has been observed in some cases.
- Postural Factors: Consistent lateral sleeping positions in infancy may exacerbate or contribute to deformity.
Ear molding devices can be effective when started early due to the temporary estrogen-induced softness of neonatal cartilage.
Auricular Anatomy
The auricle is divided into subunits: helix, antihelix, concha, and lobule. Accurate subunit identification is essential for tailored surgical correction.
Embryology
- Developmental Origin: The auricle arises from six hillocks — three from the mandibular arch (forms tragus, helical crus) and three from the hyoid arch (forms 85%, including helix, antihelix, lobule).
- Timing: Antihelical folding occurs between 12-16 weeks gestation; incomplete folding can cause prominent ear deformity.
- Structure: Made of elastic cartilage with thin skin; divided into subunits important for surgical planning.
Auricular Subunits and Landmarks
For surgical analysis, the auricle is divided into four anatomical subunits (A–D), assessed from the periphery inward. This aids in identifying deformities and selecting appropriate techniques.
- Subunit A: Helical rim and scapha — the outer contour of the ear.
- Subunit B: Antihelix — the inner ridge, often deficient in prominent ears.
- Subunit C: Conchal bowl — includes cymba and cavum, adjacent to the auditory canal.
- Subunit D: Lobule — the soft, cartilage-free lower portion of the auricle.
These key auricular landmarks are illustrated below.
Begin assessment from Subunit A and proceed inward. Overlooking peripheral deformities (e.g., macrotia or cup ear, subunits B or C) may result in incomplete or unnatural correction.
Clinical Assessment of Prominent Ear
Evaluation includes auricular measurements and analysis of subunit-specific abnormalities. Algorithmic assessment guides surgical planning.
The external ear anatomical subunits should be examined in a concentric fashion, from the outermost to the innermost.
- Subunit A - Helical & Scaphal Region: Look for flattening of the helix (folding defects) or excessive scaphal width (macrotia).
- Subunit B - Antihelical Fold: Assess the degree of cartilage folding between the triangular fossa and antitragus.
- Subunit C - Conchal Bowl (Cymba + Cavum): Evaluate the depth and projection of the concha from the mastoid.
- Subunit D - Lobule: Inspect for hypertrophy, eversion, poor definition, or bifid lobe.
The clinical presentation of otapostasis is illustrated below.
Objective Measurements
Normal auricular measurements serve as essential reference points in the preoperative evaluation. These measurements are summarised below.
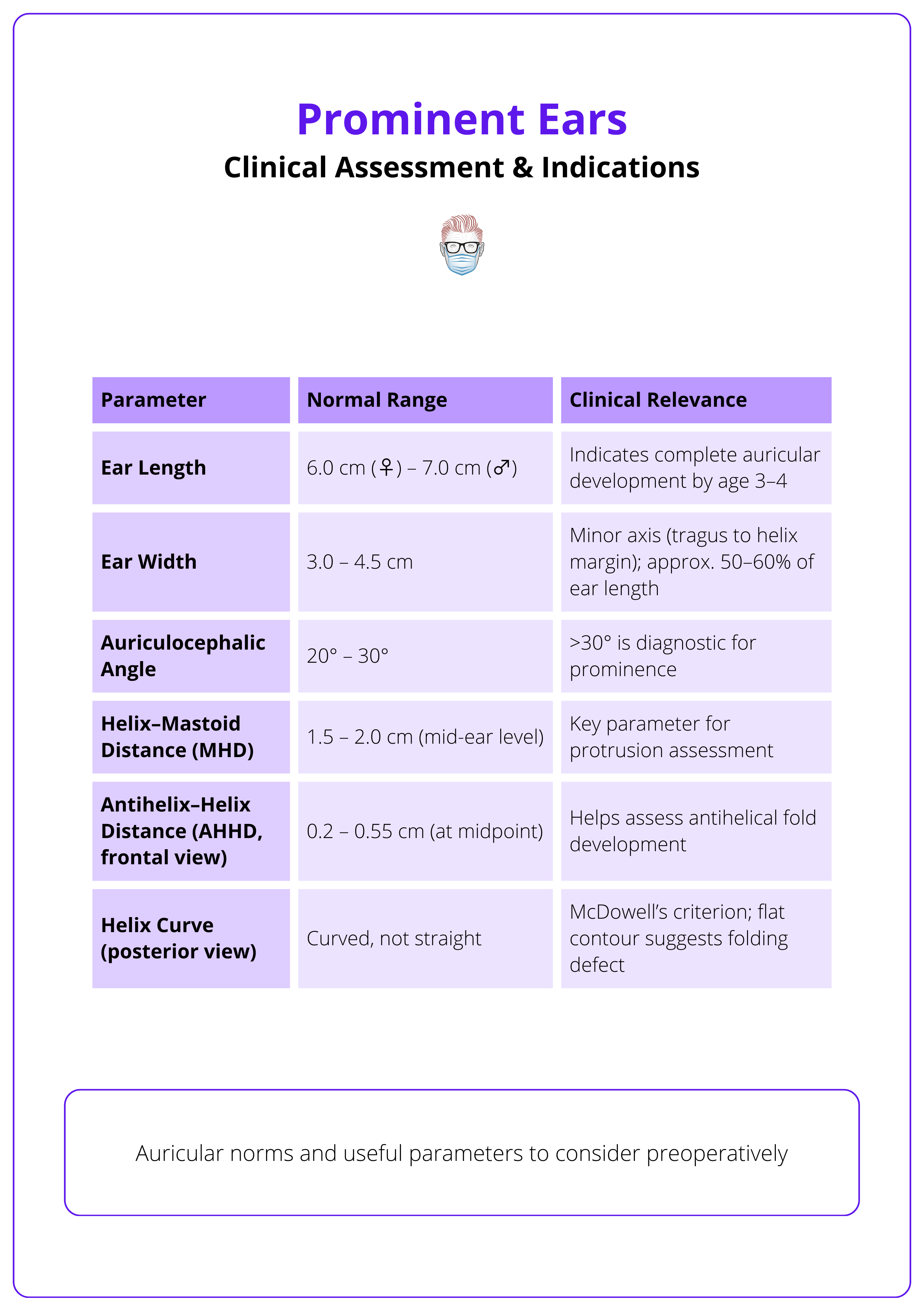
The helical rim naturally protrudes more as it descends, about 10-12 mm in the upper third, 16-18 mm in the middle, and up to 20-22 mm in the lower third!
Decision Making for Prominent Ear Treatment
Effective correction of prominent ears relies on identifying the dominant anatomical deformity and selecting a tailored surgical technique.
Prominent ear correction requires identifying the underlying deformity (e.g., antihelical underdevelopment, conchal hypertrophy) and applying targeted techniques. This ensures balanced, aesthetic results without overcorrection.
Indications
- Ear projection >2 cm or auriculo-cephalic angle >30°.
- Poorly formed antihelical fold and/or enlarged concha.
- Patient concern, psychosocial impact, or bullying.
- Auricular maturity (typically ≥3–4 years old).
Timing
- Best performed after age 3–4, when ear growth is nearly complete.
- Early correction is safe and does not impair further development.
Technique Selection
This is based on dominant deformity and discussed in more detail in the section below.
- Mustardè for antihelical fold creation.
- Furnas for conchal setback.
- Converse/Argamaso for combined or complex corrections.
By age 3-4, the external ear reaches approximately 85% of its adult size.
Surgical Technique (Otoplasty) for Prominent Ear
A subunit-based surgical approach allows tailored correction of prominent ears using techniques like Mustardè, Converse, Argamaso, and Furnas for natural, balanced results.
Prominent ear correction is optimized by assessing specific auricular subunits (A–D) and selecting techniques accordingly. This strategy helps avoid overcorrection and ensures aesthetic outcomes.
Subunit A – Helical and Scaphal Region
Target: Flat helix, excessive folding (cup ear), or macrotia due to scaphal hypertrophy.
Preferred Approach: Anterior
- Lykoudis Technique: Radial incisions to contour a flat helix; non-absorbable sutures maintain shape.
- Tanzer Correction: Reshapes excess cartilage in cup ear deformity.
- Argamaso Technique: For macrotia; wedge excision of scaphal cartilage with helical advancement.
The need for an anterior approach in Subunit A defects dictates the approach to Subunits B and C as well.
Subunit B – Antihelical Fold
Target: Insufficient or absent antihelical folding.
Preferred Approach: Posterior (unless combined with Subunit A).
- Mustardè Technique: Posterior mattress sutures create a fold; ideal for soft cartilage.
- Converse Technique: Cartilage incisions from behind to aid folding in firmer cartilage.
- Chongchet/Stenstroem Techniques: Posterior cartilage scoring to induce curvature.
Scoring techniques rely on the Gibson (and Davis) Principle: cartilage warps away from the injured side, enabling reshaping.
Subunit C – Auricular Concha
Target: Conchal hypertrophy (cymba or cavum).
Preferred Approach: Posterior (or anterior if combined with Subunit A).
- Furnas Sutures: Anchor concha to mastoid fascia to reduce projection.
- Horlock Fascial Flap: Reinforces support and vascularity, reducing recurrence risk.
- Cartilage Resection/Scoring: Directly reduces and reshapes the conchal bowl.
Subunit D – Lobule
Target: Lobular prominence, poor definition, or redundancy.
Preferred Approach: Posterior or anterior (technique-dependent).
- Lobule Suspension: Anchoring to mastoid fascia to prevent "telephone ear."
- Wedge/Curvilinear Excision: Removes excess tissue.
- Y-V Setback Technique: Advances skin and rotates lobule medially for symmetry.
Non-operative Management
In neonates ≤72 hours old, auricular cartilage remains pliable due to maternal estrogens. Splinting with materials such as SteriStrips, rubber-coated wire, or polyethylene suction catheters can realign auricular shape if maintained for 1–2 months.
This early intervention can correct prominent ears non-surgically and should be considered in perinatal assessments.
Post-operative Care & Complications of Prominent Ear
Postoperative otoplasty care includes short-term compression, soft headband use, antibiotics, activity restrictions, and monitoring for complications like hematoma and wound dehiscence.
Postoperative care is a critical component of successful otoplasty and directly impacts surgical outcomes, patient satisfaction, and complication rates.
- Immediate Care
- Compression dressing applied intraoperatively.
- Dressing removal after 24-48 hours.
- Application of a soft, non-compressive headband for 2-4 weeks, worn continuously for the first week, then at night only.
- Medications
- Prophylactic antibiotics (e.g., cefazolin IV during hospitalization; cefixime PO post-discharge for 5 days).
- Analgesics as needed.
- Elevation of the head to reduce edema.
- Activity Restrictions
- Avoid physical activities or trauma to the ears for at least 3-4 weeks.
- Return to school or light activity after 7-10 days.
Common Complications
- Hematoma: Early recognition is crucial. It may require prompt surgical evacuation to avoid vascular compromise and eventual skin necrosis.
- Suture Extrusion: More common with non-absorbable suture; minimized with proper technique.
- Overcorrection: Can result in an unnatural, "pinned-back" appearance.
- Asymmetry: Typically mild; requires careful intraoperative planning.
- Wound Dehiscence: Rare, managed with conservative wound care or minor revision.
- Recurrence of Protrusion: Often due to undercorrection or cartilage memory.
- Infections: (e.g., by Staphylococcus or Streptococcus) are managed with IV antibiotics and topical mafenide acetate if chondritis risk is high.
- Telephone Ear: Occurs when upper and lower thirds protrude after isolated mid-third correction. Results in a receiver-like deformity.
Conclusions
1. Overview: Otoplasty corrects prominent ears, usually caused by underdeveloped antihelical fold and/or conchal hypertrophy, improving auricular shape and reducing ear projection.
2. Relevant Anatomy: The auricle consists of helix, antihelix, concha, and lobule subunits. Precise identification of these areas is crucial for tailored surgical correction.
3. Clinical Assessment & Indications: Assessment includes auricular measurements and subunit-specific deformities. Surgery is indicated for ears projecting >2 cm or angle >30°, with psychological impact or patient request.
4. Surgical Techniques: Techniques such as Mustardè, Converse, Argamaso, and Furnas are adapted to the dominant deformity based on the affected subunit, aiming for natural, symmetric results.
5. Postoperative Care & Complications: Care involves compression dressings, headband use, antibiotics, activity restriction, and monitoring for hematoma, suture extrusion, asymmetry, and wound issues.
Further Readings
- Kelley P, Hollier L, Stal S. Otoplasty: evaluation, technique, and review. J Craniofac Surg. 2003 Sep;14(5):643-53. doi: 10.1097/00001665-200309000-00008. PMID: 14501322.
- Siliprandi M, Battistini A, Agnelli B, Bandi V, Vinci V, Lisa A, Maione L, Siliprandi L. Algorithm-Assisted Decision Making in Otoplasty. Aesthetic Plast Surg. 2022 Feb;46(1):207-219. doi: 10.1007/s00266-021-02368-3. Epub 2021 Jun 8. PMID: 34105004.
- Gibson T, Davis WB. The distortion of autogenous cartilage grafts: Its cause and prevention. British Journal of Plastic Surgery. 1957:257-274. doi:10.1016/s0007-1226(57)80042-3
- STENSTROEM SJ. A "NATURAL" TECHNIQUE FOR CORRECTION OF CONGENITALLY PROMINENT EARS. Plast Reconstr Surg. 1963 Nov;32:509-18. PMID: 14078273.
- CHONGCHET V. A METHOD OF ANTIHELIX RECONSTRUCTION. Br J Plast Surg. 1963 Jul;16:268-72. doi: 10.1016/s0007-1226(63)80120-4. PMID: 14042756.
- MUSTARDE JC. The correction of prominent ears using simple mattress sutures. Br J Plast Surg. 1963 Apr;16:170-8. doi: 10.1016/s0007-1226(63)80100-9. PMID: 13936895.
- Mustardé JC. The treatment of prominent ears by buried mattress sutures: a ten-year survey. Plast Reconstr Surg. 1967 Apr;39(4):382-6. PMID: 5336910.
- Furnas DW. Correction of prominent ears by conchamastoid sutures. Plast Reconstr Surg. 1968 Sep;42(3):189-93. doi: 10.1097/00006534-196809000-00001. PMID: 4878456.
- Spira M, McCrea R, Gerow FJ, Hardy SB. Correction of the principal deformities causing protruding ears. Plast Reconstr Surg. 1969 Aug;44(2):150-4. PMID: 5799297.
- Lykoudis EG, Seretis K, Spyropoulou GA. A 6-year experience in flat helix correction with a simple procedure. Arch Facial Plast Surg. 2011 May-Jun;13(3):168-72. doi: 10.1001/archfacial.2011.31. PMID: 21576663.
- Tanzer RC. The constricted (cup and lop) ear. Plast Reconstr Surg. 1975 Apr;55(4):406-15. PMID: 1118500.
- Argamaso RV, Lewin ML. The lateral transhelical approach for correction of deformities of the external ear. Aesthetic Plast Surg. 1978 Dec;2(1):357-62. doi: 10.1007/BF01577972. PMID: 24173864.
- CONVERSE JM, WOOD-SMITH D. Technical details in the surgical correction of the lop ear deformity. Plast Reconstr Surg. 1963 Feb;31:118-28. doi: 10.1097/00006534-196302000-00002. PMID: 14022738.
- Horlock N, Misra A, Gault DT. The postauricular fascial flap as an adjunct to Mustardé and Furnas type otoplasty. Plast Reconstr Surg. 2001 Nov;108(6):1487-90; discussion 1491. doi: 10.1097/00006534-200111000-00005. PMID: 11711914.
- Gosain AK, Recinos RF (2003) A Novel Approach to Correction of the Prominent Lobule during Otoplasty. Plast Reconstr Surg 112(2):575–583
