
In this week's edition
- ✍️ Letter from P'Fella
AI in surgery: Where do we draw the line? - 🖼️ Image of the Week
The tripod theory for nasal tip support. - 🚑 Technique Tip
Open rhinoplasty - structural approach. - 📖 What Does the Evidence Say?
Lateral osteotomy in rhinoplasty - 🔥 Articles of the Week
Rhinoplasty: Preservation vs structure, septal cartilage availability, & osteotomy selection. - 💕 Feedback
Suggest ideas & give feedback!
A Letter from P'Fella
AI in Surgery: Where Do We Draw the Line?
The question I have now is: if a surgeon asks, “Which one of these tools should I trust?” who can actually answer that properly?
This article I recently came across put it well. Medicine now has a crowded market of clinician-facing AI tools, but no real independent scoreboard telling us which ones are safest or most reliable.
And that’s not just a philosophical problem. A 2025 JAMA systematic review looked at over 500 studies on medical AI and found that only a tiny proportion actually used real patient care data. Most were still testing performance on exam-style questions rather than real-world clinical scenarios. So while accuracy claims are everywhere, evidence that reflects how these tools behave in actual practice is still limited.
In other words, we are producing lots of accuracy claims, but not nearly enough evidence that reflects how these tools would behave in the messy, real-world workflow of clinical care.
Plastic surgery is no different. Reviews in hand surgery and broader plastics literature describe real potential in imaging, prediction, planning, and education, but most studies remain small, retrospective, and single-centre, with limited external validation. Even when models perform well, they often drop off when tested outside the environment they were built in.
Where AI does seem genuinely helpful is in very specific parts of the workflow. Pre-operative planning, for example, where better imaging or anatomical mapping can improve efficiency and precision. Or risk prediction, where models can support counselling and expectation-setting. Burns literature suggests similar roles in assessment and monitoring. But these are all assistive roles, not replacements for judgment.
So to me, the real question is not whether AI is useful. It clearly can be. The real question is where it should sit in the surgical workflow and what level of evidence should be required before we let it sit there comfortably. In plastics, that means AI helps with pattern recognition, imaging, planning, literature retrieval, risk estimation, and repetitive admin. It probably means being much more cautious when the task starts to look like judgment, prioritization, or decision-making under uncertainty.
Medicine doesn’t just need more AI tools. It independent head-to-head benchmarking with validation and prospective testing. In a specialty like ours, “pretty good” is not a standard. If a tool is going to shape how surgeons think, plan, or counsel patients, then it should be judged like a medical intervention.
Until then, the most sensible position is probably this: stay curious, use the parts that genuinely help, and don’t confuse fluency with trustworthiness.
How are you actually using AI right now? Where do you trust it and where do you hesitate?
With love,
P’Fella ❤️
Image of the Week
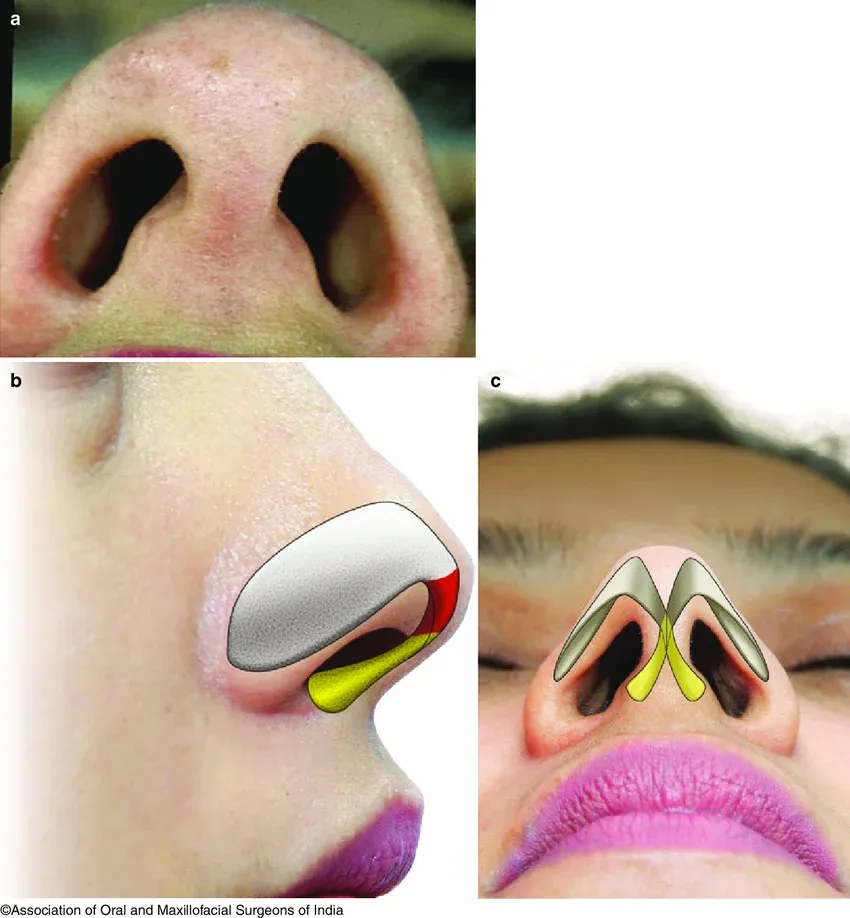
The Tripod Theory for Nasal Tip Support
This image illustrates the tripod theory of nasal tip support, a concept in rhinoplasty.
The nasal tip is supported by three components: the paired lateral crura and the central medial crura. Together, they function as a tripod, altering the length or position of any limb changes tip projection and rotation. Shortening the lateral crura increases rotation, while modifying the medial crura affects projection and columellar support.
👉 Tip position is engineered through the tripod.
Technique Tip
Open Rhinoplasty - Structural Approach
This video demonstrates an open rhinoplasty approach, where the nasal skin, soft tissue envelope is elevated to expose the underlying osseocartilaginous framework. The key principle in modern rhinoplasty is that this is not a reductive procedure, but a structural one focused on reshaping and supporting the nasal framework using controlled modification and grafting.
The critical technical takeaway is precise framework control: careful elevation, preservation of key support structures, and targeted cartilage modification (tip work, dorsal adjustment, graft placement). Successful rhinoplasty depends on maintaining or reconstructing structural support while achieving aesthetic goals, as imbalance can lead to functional compromise or long-term deformity.
What Does the Evidence Say?
Lateral Osteotomy in Rhinoplasty
When the papers directly compare technique, the signal generally favours a controlled external/perforated osteotomy over a continuous internal approach. In the Rohrich cadaver study, summarized in their later update, mucosal tearing was far less common with the external perforated technique than with the internal continuous technique (11% vs 74%). A larger clinical/cadaver series likewise reported that edema and ecchymosis were less severe, fracture-line control was excellent, mucosal injury was lower, and visible cutaneous scarring was essentially absent by 1 month with the external approach.
Most of the supporting literature is anatomic, cadaveric, and retrospective rather than high-level randomized evidence. But taken together, it supports an osteotomy strategy that is function-preserving, small-osteotome based.
Sources: (Webster, 1977); (Becker, 2000); (Giacomarra, 2001); (Rohrich, 2003); (Rohrich, 1997)
Articles of the Week
3 Interesting Articles with One-Sentence Summaries
Modern rhinoplasty is increasingly about selective preservation as top surgeons advocate blending preservation and structural techniques to maintain function, optimise 3D nasal anatomy, and improve teachability.
In rhinoplasty, harvestable septal cartilage is frequently insufficient with only ~9% of patients having adequate length for a full dorsal onlay graft, and external nasal dimensions do not reliably predict septal cartilage volume.
In rhinoplasty, medial oblique osteotomies positioned at the lateral aspect of the open roof apex achieve greater dorsal width reduction and may obviate the need for lateral osteotomies in cases of isolated dorsal widening.
