

Summary Card
Definition of Camptodactyly
Progressive flexion deformity of the PIPJ.
Features of Camptodactyly
Often bilateral and little finger. An X-Ray may show secondary complications.
Classification of Camptodactyly
Classified based on onset of deformity and severity of the flexion.
Management of Camptodactyly
Serial splinting and education for most patients. Surgery has a low success rate.
Definition of Camptodactyly
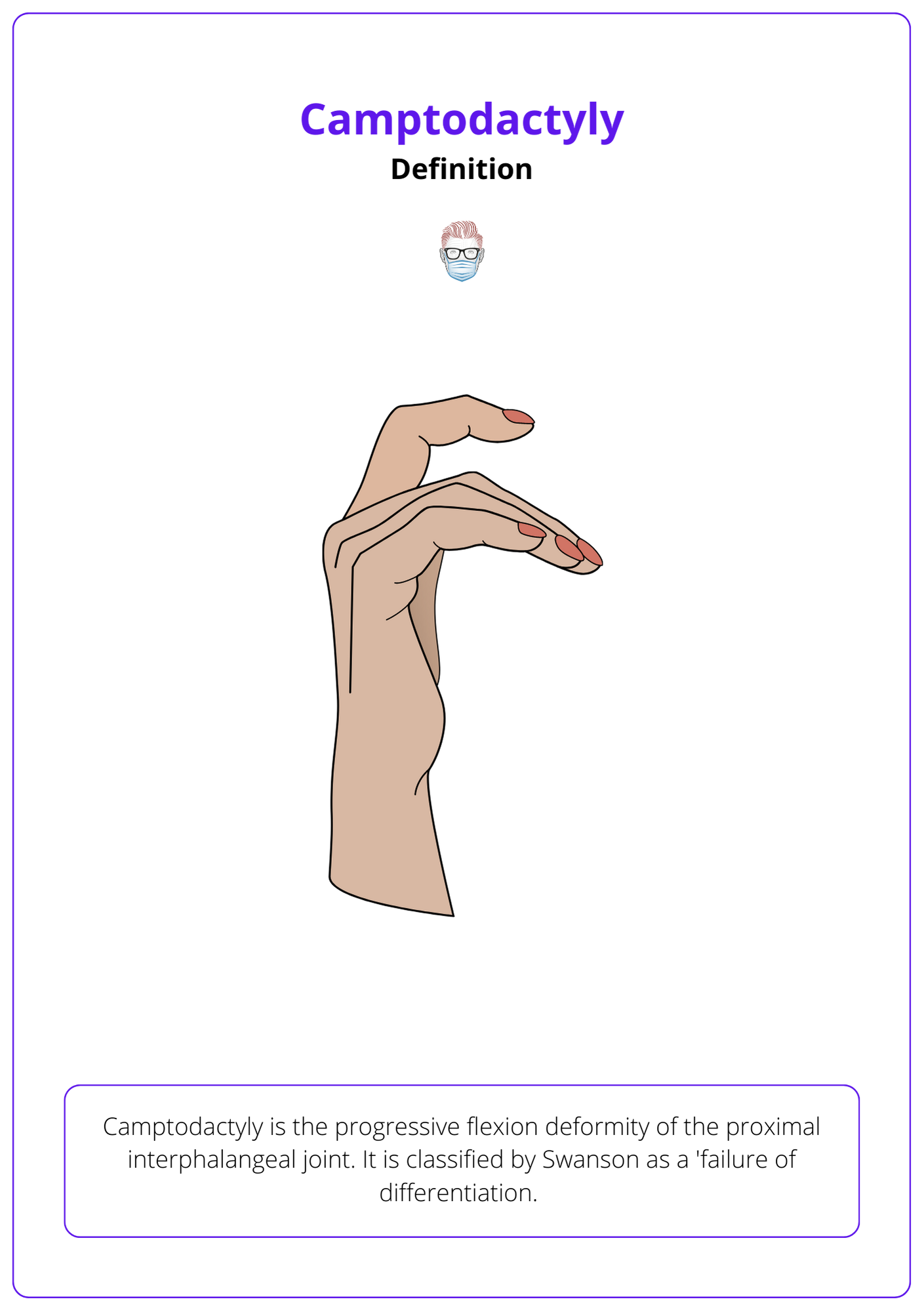
Camptodactyly is the progressive flexion deformity of the proximal interphalangeal joint. Swanson classifies it as a 'failure of differentiation'.
The image below illustrates the definition of Camptodactyly.
Features of Camptodactyly
Camptodactlyly is a flexion deformity of the PIPJ that is usually the little finger and bilaterally. Radiology may show secondary sequelae. It is classified based on the onset of deformity.
Clinical Features
Camptodactyly is characterised by the progressive flexion deformity of the proximal interphalangeal joint. It affects females more than males.
Some key points include:
- Abnormal flexion posture of PIPJ.
- Painless without swelling.
- Often bilateral and involves the little finger.
Often caused by abnormal lumbrical insertion (HINT: pain on passive extension), short FDS tendon, and abnormal extensor mechanism.
The differential diagnosis includes:
- Traumatic PIPJ injury.
- Arthrogryposis: congenital, ulnar deviation, multiple joints.
- Symphalangism (failure of joint formation) if no skin creases.
- Kirner’s deformity is not a differential diagnosis. This is a skeletal deformity characterised by progressive palmar and radial curvature of the DIPJ.
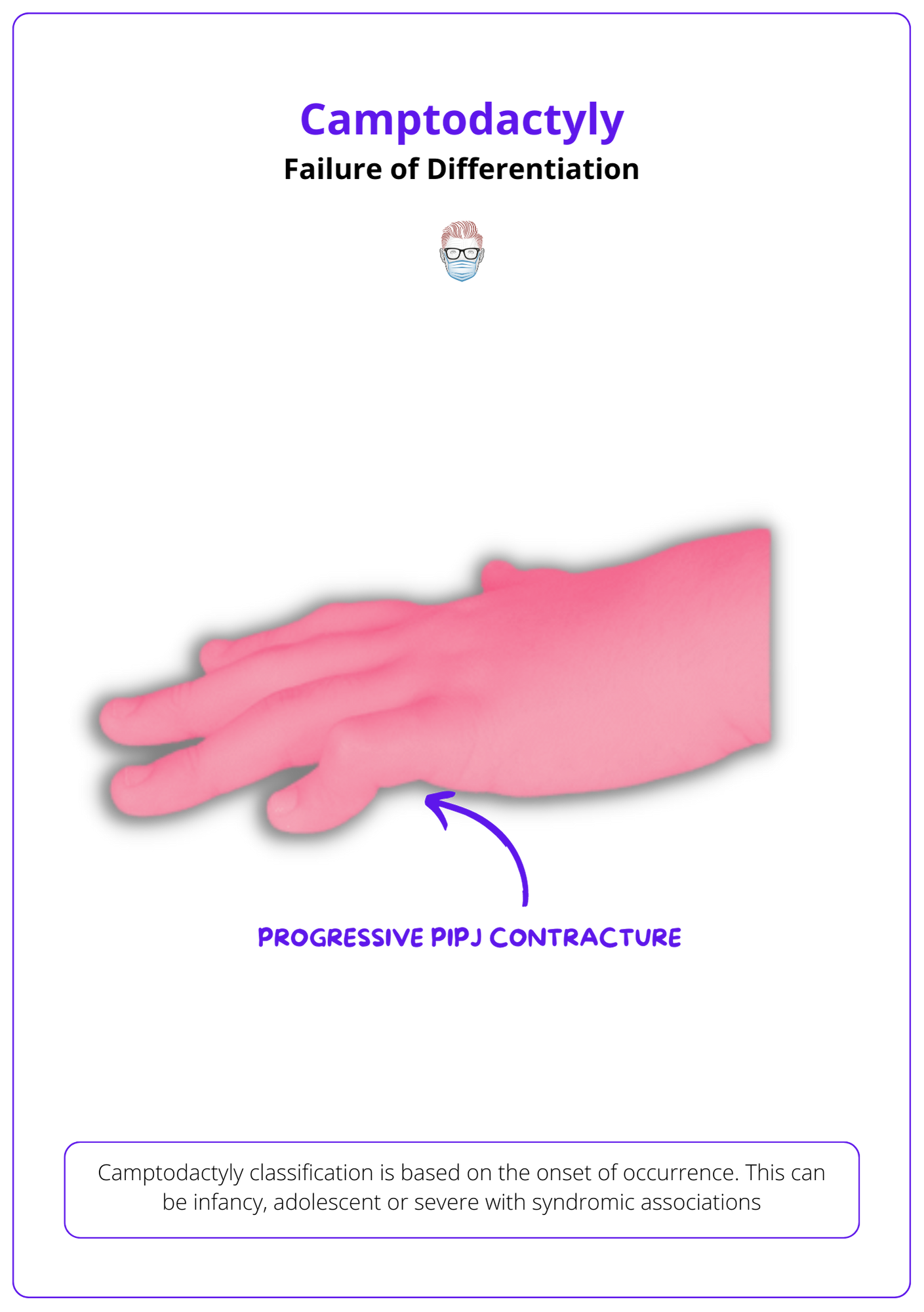
The image below illustrates this failure of differentiation of Camptodactyly.
Radiological Signs
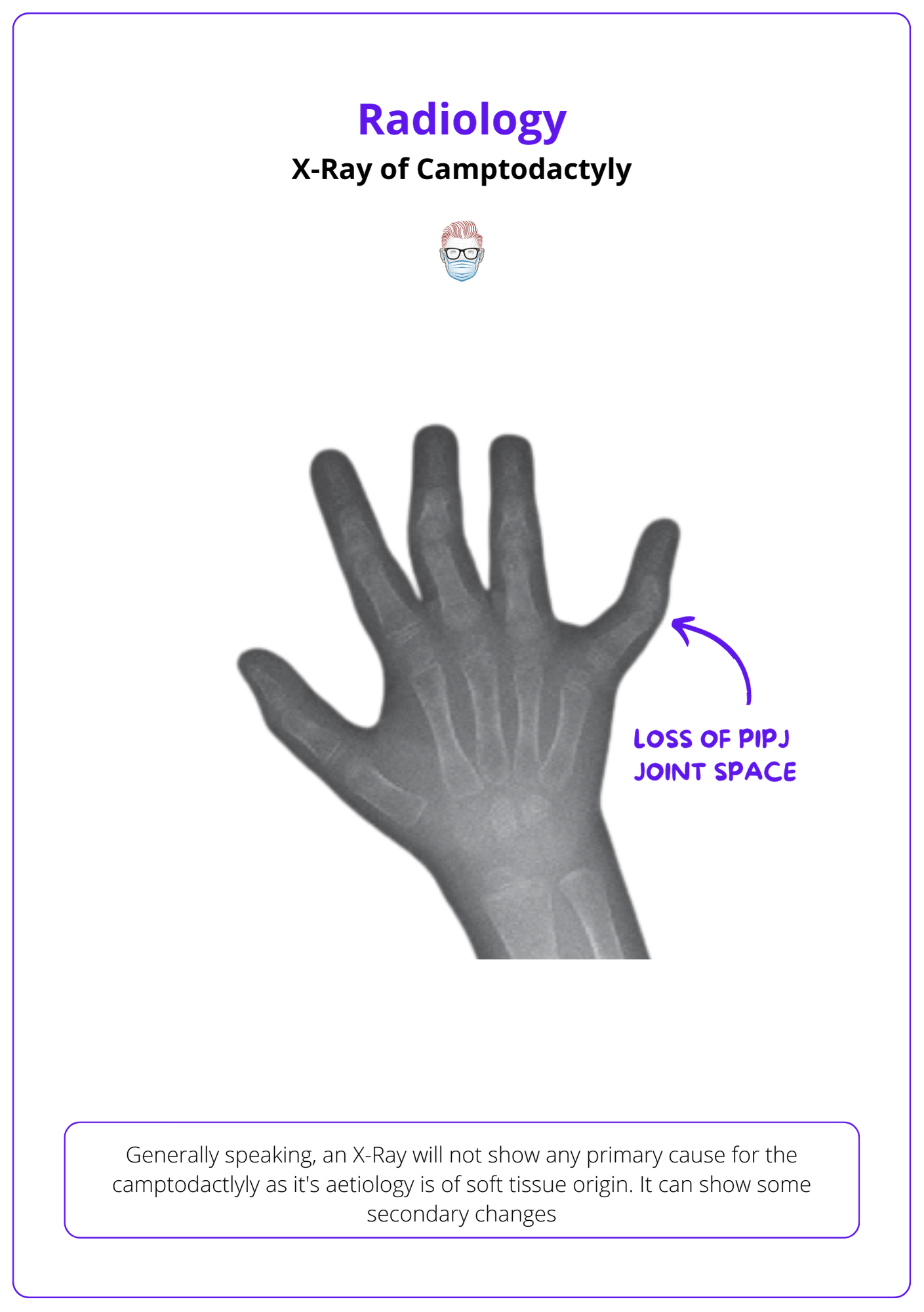
Generally speaking, an X-Ray will not show any primary cause for the camptodactyly as its aetiology is of soft tissue origin. It can show some secondary changes, such as:
- Morphological changes to the proximal phalanx.
- Decrease in proximal phalanx head convexity.
- Flattening at the base of the middle phalanx.
- Loss of PIPJ joint space with volar subluxation.
Check out the below image for the X-ray view of Camptodactyly.
Classification of Camptodactyly
Camptodactyly is classified based on onset of deformity and severity of the flexion.
Camptodactyly classification is based on the onset of flexion deformities.
- Type I: occurs during infancy (the most common type).
- Type II: occurs during pre-teenage years.
- Type III: severe, multiple digits, associated with syndromes.
Management of Camptodactyly
The majority of the patients with camptodactyly can be treated conservatively with splinting and education. Surgery is unlikely to achieve a successful outcome.
Patients with camptodactyly can be treated by conservative or surgical options. This depends on the extent of their severity.
The majority of patients can be managed in an outpatient setting by:
- Education
- Physiotherapy
- Serial Splinting or casting
In a select number of patients with severe disease, surgical considerations can include:
- FDS transfer to extensor surface
- Angulation osteotomy
- Fusion
Surgery should be performed in a step-wise manner to release and reconstruct structures until the flexion deformity is corrected.
Conclusion
1. Pathophysiology of Camptodactyly: You have learned that camptodactyly is characterized by a progressive flexion deformity of the proximal interphalangeal joint (PIPJ), predominantly affecting the little finger and often presenting bilaterally.
2. Clinical and Radiological Features: You are now familiar with the clinical presentation of camptodactyly, which typically includes a painless, abnormal flexion posture of the PIPJ without swelling, and how radiology can show secondary changes but not the primary cause due to its soft tissue origins.
3. The Classification System: You understand the classification of camptodactyly based on the onset of the deformity and the severity of the flexion for predicting the progression and planning the management strategy.
4. Management Strategies: You have understood the conservative management approaches such as education, physiotherapy, and serial splinting, and understand when surgical intervention might be considered, and its generally low success rate.
