

Summary Card
Pathophysiology of Electrical Burns
Electrical burns lead to thermal heating, electroporation, and protein denaturation, with severity determined by the current, voltage, and resistance formula.
Types of Electrical Burns
Electrical burns can be classified as high or low voltage, direct or alternating current.
Lightning Strike Burn
Lightning is an extremely high voltage, high amperage, ultra-short duration electrical discharge of direct current.
Severity of Injury
This is influenced by voltage & resistance. Bone is the most resistant and its slow heat escape results in more thermal injury (Joule Effect).
Management of an Electrical Burn
Switch off the power source, ATLS surveys, cardiac monitoring and standard burn management. It may increase urine output or fasciotomy.
Pathophysiology of Electrical Burns
Electrical burns result in thermal heating, electroporation, and protein denaturation.
An electrical burn can occur by direct contact or indirectly via an arc, flash, or flame. This results in three pathophysiological effects:
- Thermal burn via carbonation and joule heating.
- Electroportation (pors in cell membranes to allow free passage of fluid and electrolytes).
- Protein denaturation.
The degree of these mechanisms is influenced by the current, voltage and resistance. More specifically, current = voltage/resistance.
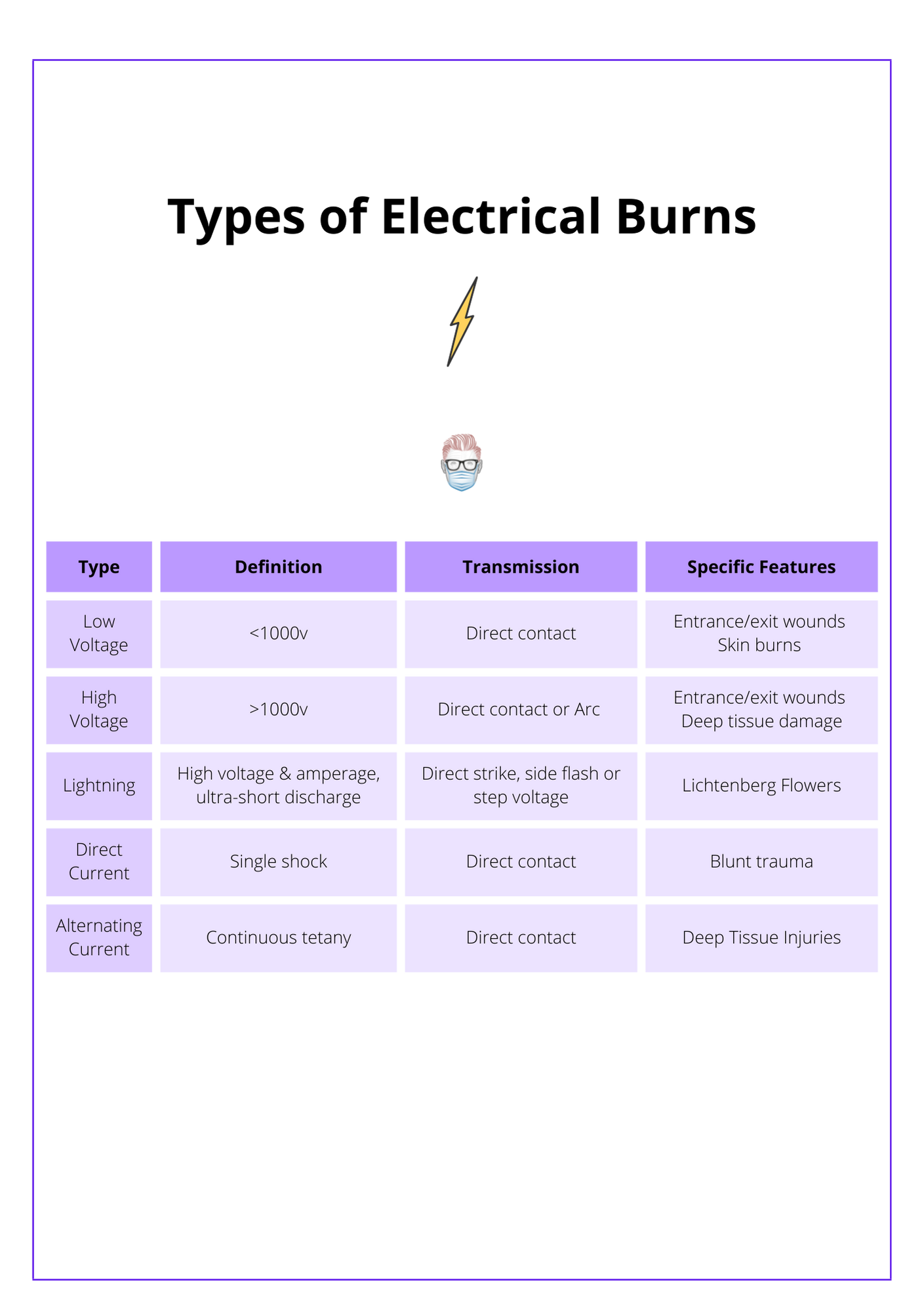
Types of Electrical Burns
Electrical burns can be classified as high or low voltage, direct or alternating current.
Electrical burns can be classified by their voltage and their type of current.
In terms of voltage, this can be a low voltage, high voltage, or lightning strike electrical burn. Currents can be described as direct (DC) or alternating (AC). This is illustrated in the diagram below.
Low Voltage Electrical Burn
A low-voltage electrical injury is defined as less than 1000 volts. The patients will have entrance and exit wounds but generally no deep tissue damage.
For example:
- Standard single-phase household electrical supply.
- Industrial power supplies are often three-phase and commonly 415 volts.
- Common car battery.
- Surgical diathermy.
High Voltage Electrical Burn
A high-voltage electrical injury is defined as more than 1000 volts. It can cause an injury through the current transmission and also flash burns.
These patients are less likely to have direct contact with the source. Instead, they are injured indirectly through an arc of flash flame.
Flash burns
- Skin burns without deep tissue damage or entrance/exit wounds.
- Current isn't transmitted through the patient.
- A high-tension discharge creates an arc or “flash over” that can ignite clothing.
Transmission Burns
- Skin burns with deep tissue damage and entrance/exit wounds.
- This is the mechanism of electroporation.
- Compartmental swelling, tenderness and pain are a sign of muscle damage that fasciotomies should be strongly considered for.
- Haemochromgens released from muscle can result in acute kidney injury.
Direct and Alternating Current
There are two types of current; direct currents (DC) and alternating currents (AC).
Direct Current
- Usually a single shock.
- The patient is thrown away from the electrical source.
- The main complication is blunt trauma but an arrhythmia may occur.
Alternating Current
- Can cause continuous muscle tetany.
- Prevents the patient from releasing their touch on the source.
- High complication rate compared to direct current injuries.
Lightning Strike Burn
Lightning is an extremely high voltage, high amperage, ultra-short duration electrical discharge of direct current.
Pattern of Injury
Lightning strikes can occur as a direct strike (high mortality), a "side flash" or "step voltage".
- Side flash occurs when lightning strikes an object of high resistance such as a tree. The current is then deflected through a victim on its way to the ground.
- Step voltage occurs when the discharge flowing through the ground may pass up one leg and down the other.
A lightning strike is illustrated in the image below.

Complications
- Lichtenberg flowers are pathognomonic of a lightning strike.
- Burns and deep muscle damage are less common than other electrical burns.
- Respiratory (discharge affecting the medullary respiratory centre).
- Cardiac arrest.
- Perforated tympanic membrane.
- Corneal damage.
Severity of Electrical Burn Injuries
The severity of electrical burn injuries depends on the electrical current's characteristics such as voltage, resistance, and contact duration, and the path electricity takes through the body.
The severity of an electrical burn is multifactorial. It is strongly influenced by the characteristics of the electrical current and the direction of the electricity travelling through the body.
Characteristics of the Electricity
The important electrical characteristics that influence the degree of injury are:
- Current: voltage x resistance.
- Resistance: more resistant anatomy creates more thermal energy.
- Duration of contact.
Different tissues exhibit characteristic electrical resistance according to their electrolyte content. The most resistant are ordered below.
- Bone: slow heat escape can cause secondary thermal damage (Joule Effect).
- Skin: increased in thick, dry skin.
- Fat: once the skin is breached, fat receives an increased current.
- Nerve: can be secondary thermal damage as heat is slow to escape from bone.
- Muscle: will result in oedema, myoglobinuria and hyperkalemia.
- Blood and fluid: the least resistance anatomical structure.
Entry and exit wounds of electrical burns are illustrated below.
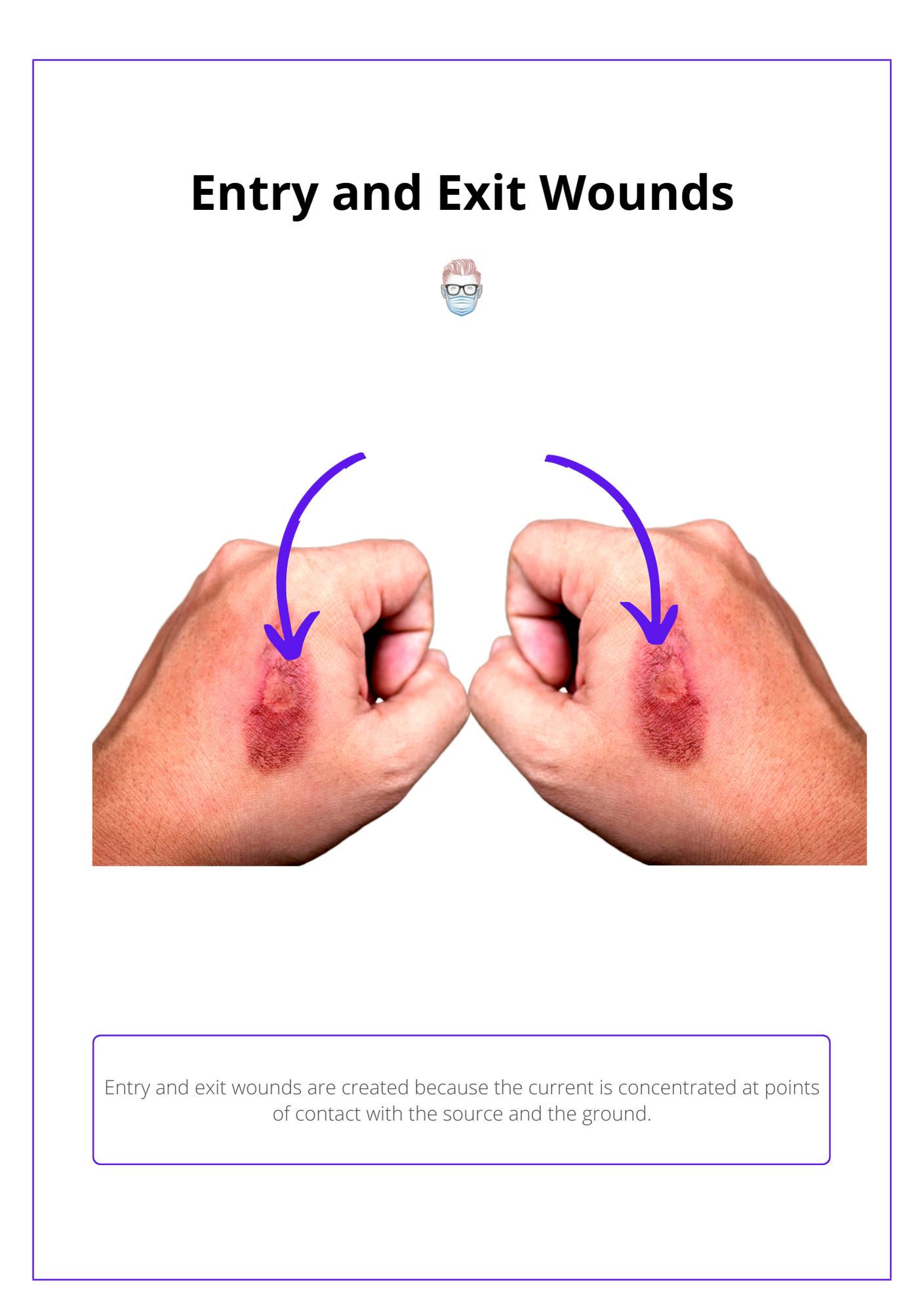
Direction of Electricity
The direction of the electrical conduction provides a guide for the type of burn injury. For example:
- Chest: cardiac arrest, myocardial damage, ventricular fibrillation, or delayed arrhythmias.
- Brain: respiratory arrest, neurological (seizures).
- Ears: tympanic membrane.
- Eyes: corneal injury, cataracts.
Management of an Electrical Burn
Management of electrical burns involves immediate power source disconnection, adherence to ATLS protocols, and referral to burn centers.
Management of electrical burns involves immediate power source disconnection, adherence to ATLS protocols, and referral to burn centers. Treatment focuses on specialized fluid resuscitation, cardiac monitoring, potential fasciotomies for high-voltage injuries, and aggressive management of myoglobinuria with diuretics to prevent renal complications from rhabdomyolysis.
Basic Management
- Switch off the power source and avoid personal injury.
- ATLS guidelines with a primary survey, secondary survey, AMPLE history.
- Referral to Specialist Burn Centre to treat burns.
Specific to Electrical Burns
Fluid Resuscitation
- Standard burns resuscitation formula may be inadequate.
- Haemochromogenuria requires a urine output of 75–100ml/hr in adults, and 2ml/kg/hr in children until urine is clear.
Cardiac
- Treat cardiac and respiratory arrest.
- 24 hours of ECG monitoring may be required for high voltage injury, loss of consciousness, or abnormal ECG on arrival.
Fasciotomy
- High voltage injury involving limbs may require fasciotomy.
- Resuscitate prior to fasciotomy so that haemochromogens from the newly perfused muscle are flushed rapidly through the kidneys.
- Intra-operative hypotension can result in delayed haemorrhage.
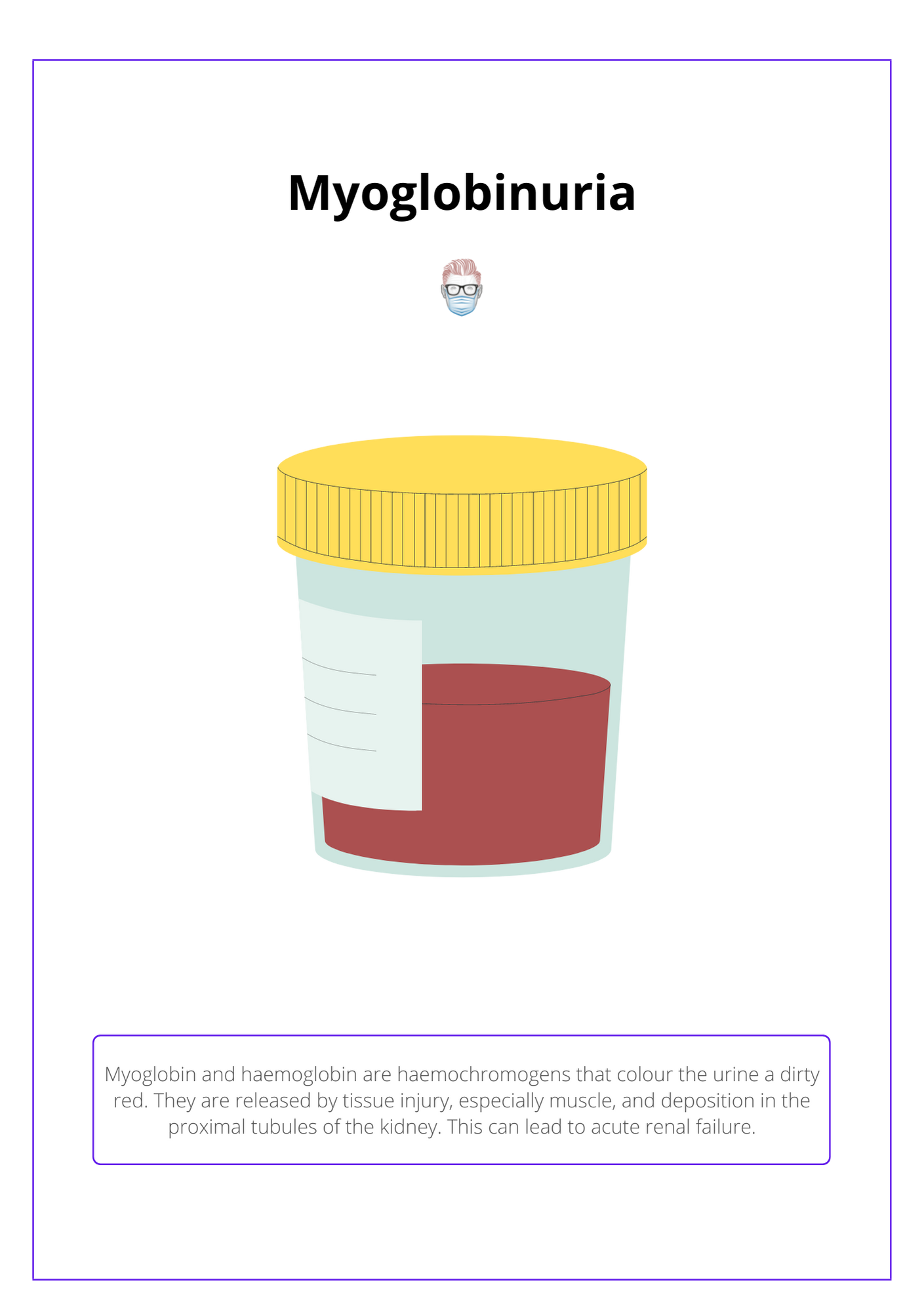
Myoglobinuria
- Haemochromogens suggestive of rhabdomyolysis
- Intratubular deposition results in renal failure
- Increase urine output to 75-100 ml/hr in adults, 2ml/kg/hr in children
- Consider adding in mannitol, furosemide or sodium bicarbonate
The image below illustrates Myoglobinuria.
Conclusion
1. Electrical Burn Pathophysiology: You've gained insight into how electrical burns result from thermal heating, electroporation, and protein denaturation, influenced by the voltage, current, and resistance encountered.
2. Types of Electrical Burns: You understand the classification of electrical burns into high or low voltage, and direct or alternating current, which helps in anticipating the injury pattern and guiding treatment.
3. Recognizing Lightning Strike Burns: You've learned about the unique characteristics of lightning strike burns, which are high voltage and direct current events with specific injury patterns and complications.
4. Assessing the Severity of Electrical Burn Injuries: You are familiar with the factors that determine the severity of electrical burns, including the electrical current's characteristics and the path it takes through the body.
5. Management for Electrical Burns: You have explored the essential management steps for electrical burns, including immediate care, the importance of continuous monitoring, and specific interventions.
