
In this week's edition
- ✍️ Letter from P'Fella
Technique without context. - 🤓 The Sunday Quiz
*Drumroll🥁* Winner announced! - 🖼️ Image of the Week
Cadaveric injection of the posterior interosseous artery. - 🚑 Technique Tip
PIA flap for dorsal hand & first web space reconstruction. - 📖 What Does the Evidence Say?
Reverse PIA flap: When is it the right choice? - 🔥 Articles of the Week
Original PIA flap study, PIA flap for fingers, & Extending the Posterior Interosseous Artery Flap. - 💕 Feedback
Suggest ideas & give feedback!
A Letter from P'Fella
Technique Without Context
It was about reading.
Specifically: reading the work that came before you.
When we were preparing for the episode, we went back to the original publications. Not summaries. Not textbook adaptations. The actual papers.
And it’s striking.
When Claudio published in the 1980s, reconstructing the first web space wasn’t just another case on the list. Microsurgery wasn’t routine. Options were limited. Paying an “artery price” with a radial forearm flap was a real trade-off. Free tissue transfer was significant.
How does one understand the elegance of a local dorsal hand flap unless they understand the problem it was built to solve?
That context disappears if you only read modern summaries. Because techniques don’t appear fully formed. They evolve because something wasn’t working.
Flap congestion. Unreliable perforators. Tension across the web space. Poor arc of rotation. Every modification, every refinement, every step in the technique came from someone struggling with a specific limitation.
If you skip the original work, you miss that reasoning.
And if you miss the reasoning, you don’t really understand the flap. Instead, you just memorise the steps.
There’s a temptation in academic surgery to add another publication. Another small variation. Another case series.
But sometimes the better use of your time isn’t writing something new. It’s reading something old.
- Go back to the original paper.
- Read what they were worried about.
- Read what failed.
- Read what they were trying to avoid.
Your patients will benefit far more from that than from you adding one more PDF to the pile.
If you’re revisiting muscle flaps, dorsal hand flaps, or web space reconstruction, don’t just learn the steps. Learn the why. The era. The constraint.
Technique without context is just choreography. And your surgical skills deserve better than that.
With love,
P’Fella ❤️
The Sunday Quiz
*Drumroll🥁* Winner Announced!
We're thrilled to announce the winner of this edition's quiz. After seven rounds of questions on plastic surgery, our top scorer is Paul!
A huge thank you to everyone who joined us throughout the series. If you missed it, don't worry. New quizzes and challenges are already in the works!

Image of the Week
Cadaveric Injection of the Posterior Interosseous Artery
This week's image demonstrates cadaveric injection of the posterior interosseous artery (PIA), outlining the vascular territory that underpins the reverse-flow PIA flap.
The left panel shows the injected vascular network along the dorsal forearm, highlighting the consistent septocutaneous perforators. The right panel demonstrates clinical planning over the distal forearm: a common indication zone for dorsal hand defects.
The PIA flap is a distally based fasciocutaneous flap, relying on retrograde flow through the interosseous system and preserved distal anastomoses. Its key advantage is:
👉 Coverage of dorsal hand and wrist defects without sacrificing a major forearm artery.

Technique Tip
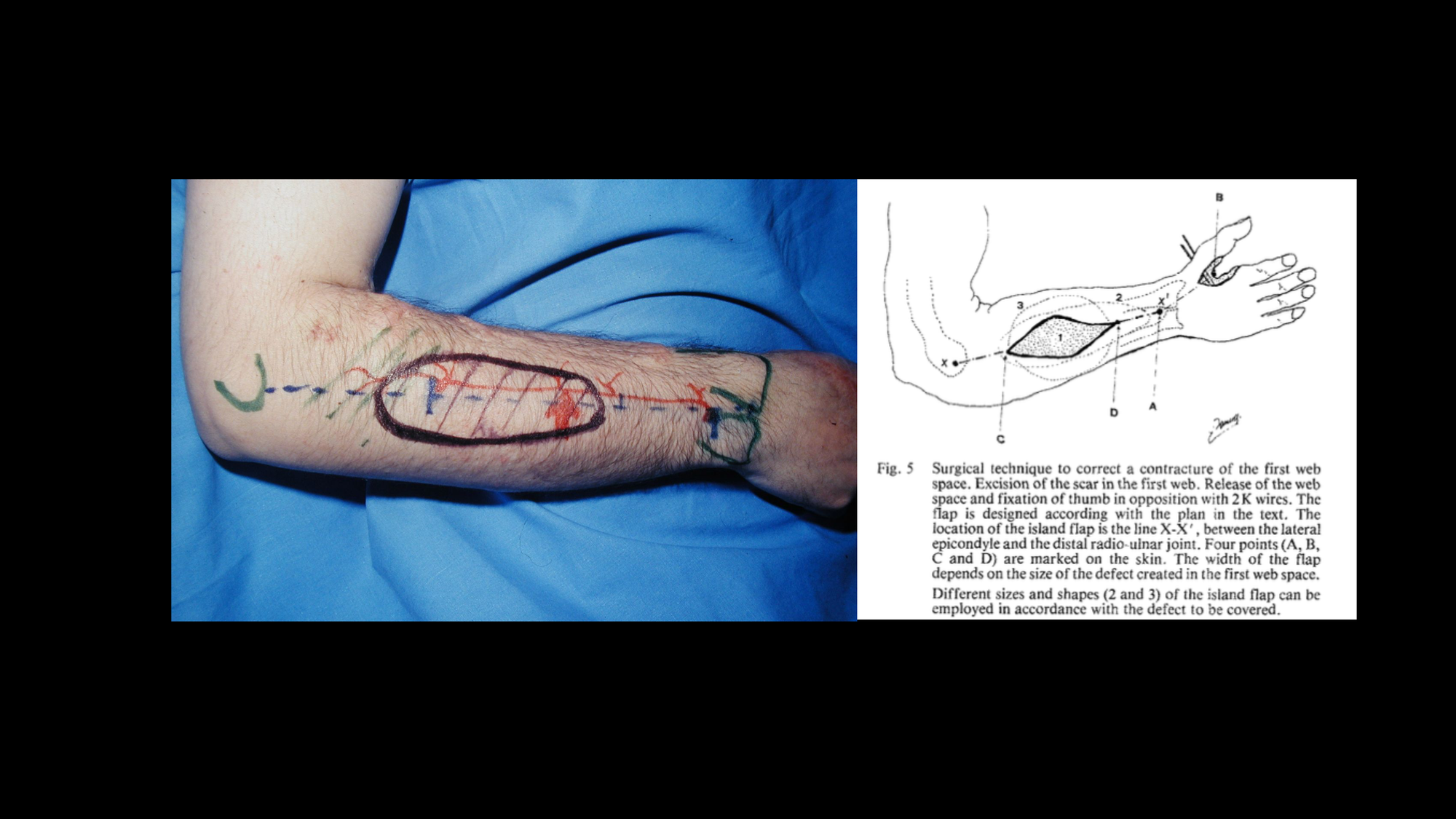
PIA Flap for Dorsal Hand & First Web Space Reconstruction
The PIA flap is a reliable reverse-flow fasciocutaneous flap ideal for coverage of dorsal hand, wrist, and first web space defects without sacrificing a major forearm vessel.
Flap Design
The flap is designed along the line between the lateral epicondyle and the distal radioulnar joint, corresponding to the course of the posterior interosseous artery within the septum between EDC and ECU.
- Mark the line from the lateral epicondyle to the distal radioulnar joint (PIA course between EDC and ECU).
- Pivot point: ~2-3 cm proximal to the DRUJ (distal AIA–PIA anastomosis).
- Design the flap proximally in the mid-forearm.
- Size according to defect and avoid overextending beyond the reliable distal pivot.
Surgical Technique
- Elevate in a subfascial plane, preserving septal perforators.
- Identify the intermuscular septum between EDC and ECU.
- Dissect and island the pedicle proximally, maintaining distal retrograde inflow.
- Transfer without kinking; avoid tight tunnels (venous congestion risk).
- Donor site usually requires skin graft.
Thin, reliable dorsal coverage while preserving major forearm vessels is ideal for traumatic or post-tumour dorsal hand defects.
Source: Claudio Agrigiani
What Does the Evidence Say?
Reverse PIA Flap: When Is It the Right Choice?
Across large clinical experience and reviews, the most supported “sweet spots” for indication are: dorsal hand defects up to the metacarpal/MCP region, first web space reconstruction (often up to the thumb IP level), and ulnar border hand defects, with additional reported utility for thumb and selected volar/dorsal traumatic defects when local options are limited.
The key decision-driver (and the reason it still gets picked over forearm options based on major axial vessels) is arterial preservation: multiple sources highlight it as particularly attractive when you want coverage but can’t justify sacrificing a main hand artery (or when the vascular situation is uncertain after injury).
Outcomes are generally strong, with contemporary reporting showing ~90%+ overall success, but the trade-off is a recognizable complication profile: most notably venous congestion and partial/rare total flap loss, plus a not-infrequent need for donor-site grafting depending on flap width/closure.
One consistent technical constraint behind “indication creep” is territory: classic anatomical/clinical work supports the concept that the reliably perfused skin territory is not unlimited (with proximal overreach increasing risk), which matters when deciding whether a defect is “in reach” for a reverse PIA versus requiring an alternative flap.
Sources: (Angrigiani, 1993), (Costa, 2001), (Cheema, 2007), (Kelada, 2022), (Cho, 2025)
Articles of the Week
3 Interesting Articles with One-Sentence Summaries
The posterior interosseous “reverse” forearm flap is a reliable distal forearm flap that is actually perfused by direct flow through the recurrent dorsal branch of the anterior interosseous artery rather than true reversed flow, making it dependable when raised within its defined vascular territory.
The posterior interosseous free flap can resurface complex finger defects without sacrificing a major hand artery, achieving 100% flap survival, direct donor-site closure, improved total active motion, and even allowing dual-paddle designs to reconstruct separate finger regions in one go.
Moving the pivot point of the classic reverse PIA flap from the anterior interosseous artery to the dorsal intercarpal arch helps gain roughly 8.5 cm of additional pedicle length, enough to extend coverage all the way to the fingertips without sacrificing a major forearm artery.
