
In this week's edition
- ✍️ Letter from P'Fella
Medicine is slowly replacing the knife. - 🤓 The Sunday Quiz
How well do you know hand compartment syndrome? - 🖼️ Image of the Week
Key compartments of the hand. - 🚑 Technique Tip
Volar forearm fasciotomy for compartment syndrome. - 📘 Foundations Textbook
Last call to grab foundations! - 🔥 Articles of the Week
Acute compartment syndrome, diagnosis and management of compartment syndrome, & Volkmann’s ischaemic contracture. - 💕 Feedback
Suggest ideas & give feedback!
A Letter from P'Fella
Medicine Is Slowly Replacing the Knife
Not because surgeons are worse, but because the biology is finally being understood.
Melanoma is the obvious example.
Wide excisions and nodes used to be the main event. Now, for many patients, immunotherapy does the heavy lifting. Surgery still matters, but more for diagnosis, staging, or local control. Completion clearance? Much less common. The centre of gravity has shifted.
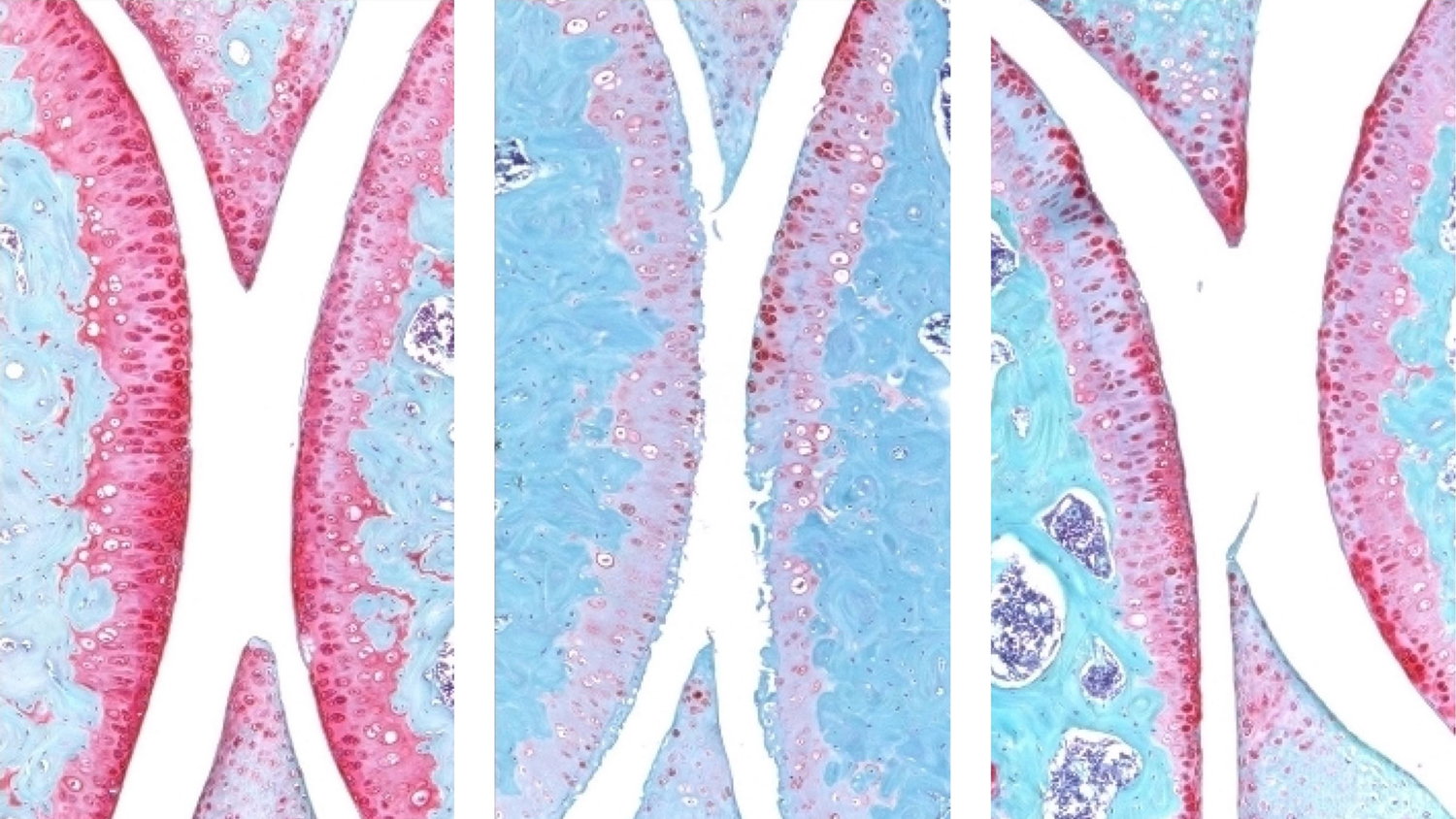
Arthritis feels similar. For years, it’s been treated as a mechanical failure: injections, symptom control, then replacement. Papers like the Stanford cartilage study hint at a different future.... arthritis as something biologically modifiable earlier, rather than something we wait to collapse before operating.
This isn’t surgery losing ground. It’s medicine moving upstream.
Plastic surgery sits in an interesting place here. We often step in when nothing else works — wounds, scars, tissue loss. But as mechanisms get clearer, medicine tends to arrive earlier, and surgery moves later.
The pattern’s familiar:
- Poor understanding → we operate
- Better biology → medicine leads
- Surgery becomes more selective
Not good or bad. Just reality. The real question isn’t “are we being replaced?”
It’s “are we paying attention early enough?”
Because the work doesn’t disappear...it just changes shape.
With love,
P’Fella ❤️
The Sunday Quiz
How Well Do You Know Hand Compartment Syndrome?
Join this round of our Weekly Quiz in each edition of thePlasticsPaper. This is the sixth round of seven rounds!
The top scorer wins our Foundations textbook at a discount!
Image of the Week
Key Compartments of the Hand
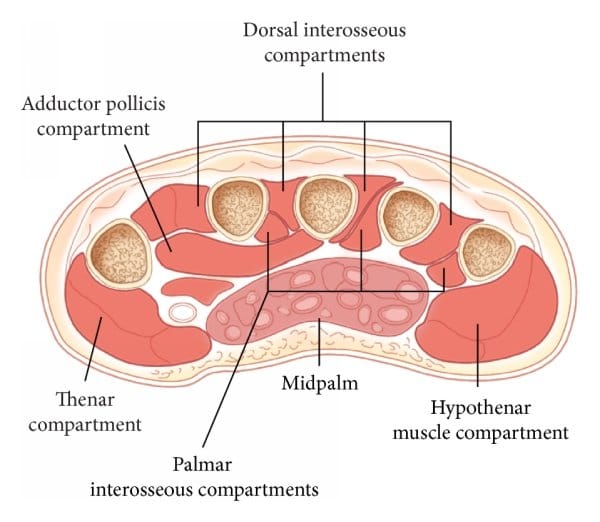
This cross-sectional diagram illustrates the key compartments of the hand: the thenar, hypothenar, midpalmar, adductor, and interosseous compartments.
In hand sepsis, infection spreads within these closed anatomical spaces, not randomly through soft tissue. This explains why dorsal swelling often originates from a palmar space, and why inadequate drainage leads to persistent infection.
👉 Successful drainage depends on identifying and decompressing the correct compartment.
Technique Tip
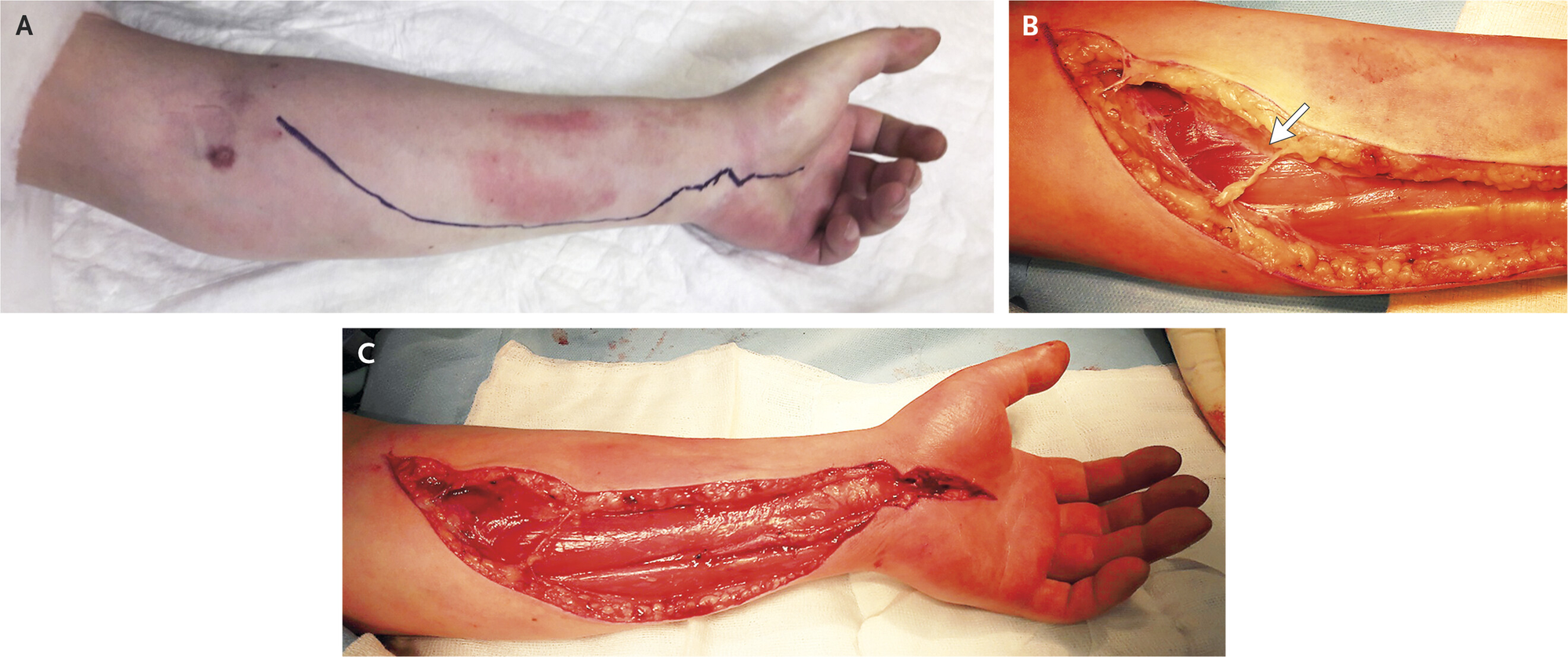
Volar Forearm Fasciotomy for Compartment Syndrome
1. Plan an extensile volar S-incision (prox forearm → wrist), positioned to preserve viable skin bridges and allow easy proximal/distal extension.
2. Raise full-thickness flaps (skin + subcut), then perform a long, continuous volar fasciotomy.
3. Release both volar compartments explicitly: superficial then deep volar (common miss); extend proximally if tethered.
4. Distal add-on: carpal tunnel release when distal swelling/reperfusion risk or median symptoms/concern.
5. If any doubt about completeness: add dorsal decompression and release mobile wad when lateral/dorsal tension persists or mechanism is crush/reperfusion/delay.
6. Dress + plan: VAC/loose dressings, second look 24-48h, document compartments + extent.
Foundations Textbook
Last Call to Grab Foundations
Foundations was designed for the reality that most learning happens in short gaps: between cases, on call, late at night, or the morning before a list. We've built it with concise lessons, anatomy that connects directly to the OR, and material you can pick up in spare moments instead of slogging through endless pages.
It’s become part of the daily routine for thousands of trainees, and we’re genuinely thankful for that.
If you’ve been considering it, this is the final window before it’s taken offline for a while again.
Articles of the Week
3 Interesting Articles with One-Sentence Summaries
Although rare, upper-extremity compartment syndrome demands rapid diagnosis and fasciotomy, as delays quickly lead to irreversible muscle necrosis and permanent limb dysfunction.
Despite modern pressure monitors and imaging adjuncts, compartment syndrome is still fundamentally a clinical diagnosis — and outcomes hinge on maintaining a low threshold for early fasciotomy rather than waiting for perfect measurements.
Management of Volkmann’s contracture is severity-dependent: mild, moderate, and severe patterns require different surgical and rehabilitative strategies rather than a single uniform approach.
