
In this week's edition
- ✍️ Letter from P'Fella
The groin was always there. The system wasn’t. - 🤓 The Sunday Quiz
Making some renovations! - 🖼️ Image of the Week
The superficial circumflex iliac artery in detail. - 🚑 Technique Tip
Modified SCIP flap (superficial circumflex iliac artery perforator). - 📖 What Does the Evidence Say?
SCIA perforator cadaver injection. - 🔥 Articles of the Week
SCIP flap for recon, groin flap for hand recon, & perforasomes. - 💕 Feedback
Suggest ideas & give feedback!
A Letter from P'Fella
The Groin Was Always There. The System Wasn’t.
But for years, it came with a trade-off: you could have reliability, or you could have refinement. Not both. The “classic” groin flap worked, but it often meant bulk, awkward inset, and a flap that didn’t always feel like it belonged in modern microsurgery.
Then the SCIP flap turned up in the 2000s and changed the mood completely.
Perforator-based. Anatomically precise. Thin on purpose.
And at some point, SCIP stopped being “an alternative” and became something people reached for without doubts.
A lot of surgeons trace that shift to one person: Professor JP Hong.
We recorded an episode of our podcast, How I Operate with him recently, and I came away thinking the same thing I’ve thought after meeting the best technical surgeons:
It’s not that they have better hands. It’s that they’ve built a system that makes good outcomes more likely, even when the day is busy and the case is moving fast.
What makes SCIP feel “predictable”
When people talk about JP Hong’s SCIP, they usually say one word: Predictable.
And the more we dug into the history, the more you realise how much of that predictability is earned.
Koshima’s original description was elegant, but anyone who has tried it early on knows the friction points show up quickly:
- Short pedicle.
- Bulk where you don’t want it.
- Vessel mismatch.
- Seroma at the donor.
- And the reputational killer: venous congestion.
What JP has done over the last two decades is take those weak points seriously, then refine the flap until it behaves with a sequence of small, deliberate decisions. The SCIP flap doesn’t become reliable because you know the anatomy. It becomes reliable because you confirm the anatomy.
Quick teaser from the podcast
Midway through the recording, I asked JP to do something that sounds simple and is actually brutal:
Describe a SCIP flap clearly enough that someone can mentally rehearse it on the way to theatre.
With no slides, no diagrams. Just words. And he did it.
And it’s exactly why this episode will be worth your time. It’s the closest thing to a practical operating manual you’ll get from the person who helped make this flap mainstream.
We’ll be releasing the episode soon as part of the new season.
The point of all this
A lot of good ideas never spread. SCIP spread because it became teachable.
With love,
P’Fella ❤️
The Sunday Quiz
Making Some Renovations!
Check back next week :)
Image of the Week
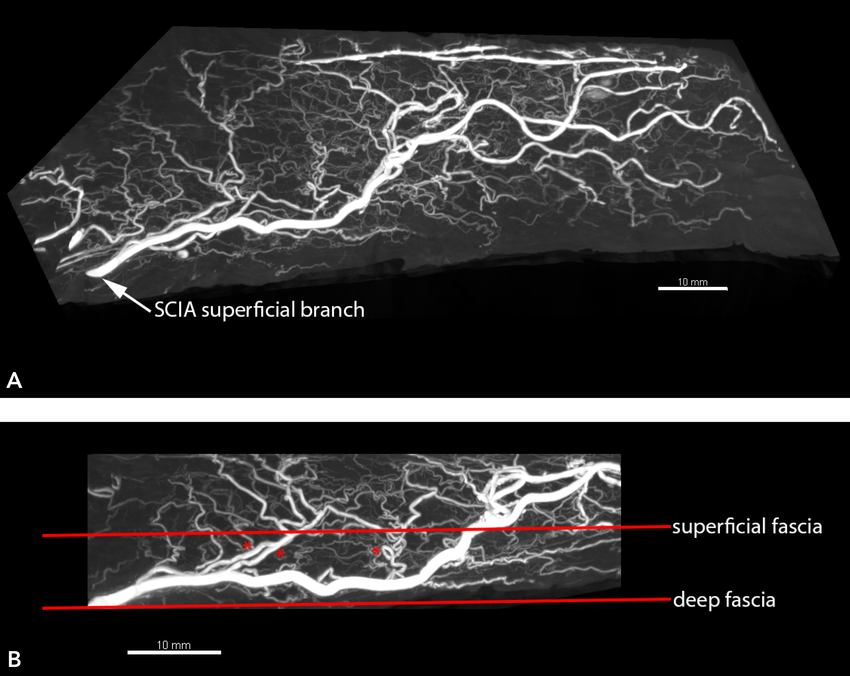
The Superficial Circumflex Iliac Artery in Detail
This image illustrates the superficial branch of the superficial circumflex iliac artery (SCIA) — the vascular foundation of the SCIP flap.
The 3D overview (A) shows the main vessel coursing laterally, while the 2D section (B) demonstrates multiple small-calibre perforators branching before one dominant perforator penetrates the superficial fascia to become the primary supply. Note the tortuous course of these vessels, which is a feature that likely contributes to the flap’s ability to tolerate rotation and inset tension.
After fascial penetration, the main perforator travels within the superficial fat, arborising into the subdermal plexus, enabling harvest of a thin, pliable perforator flap.
Technique Tip
Modified SCIP Flap (Superficial Circumflex Iliac Artery Perforator)
The SCIP flap is a thin, pliable perforator flap ideal for extremity and small soft tissue defects, with minimal donor morbidity. In the video below, J.P. Hong demonstrates elevation on the superficial fascia plane for rapid, safe harvest.
🖊️ Flap Design
- Mark along the inguinal ligament, centred over the SCIA perforators.
- Identify perforators (Doppler helpful).
- Design flap according to defect size; can be harvested thin.
- Preserve the pedicle length for microsurgical reach.
🔪 Surgical Technique
- Incise and elevate in the superficial fascia plane (relatively avascular).
- Preserve the perforator while maintaining flap thinness.
- Skeletonize the SCIA pedicle as required.
- Rapid elevation possible due to minimal bleeding in this plane.
- Donor site typically closed primarily.
What Does the Evidence Say?
SCIA Perforator Cadaver Injection
Injection + CT/micro‑CT work shows both superficial and deep branches typically provide multiple perforators, but the deep-branch pattern has greater anatomic “headroom” (larger potential flap territory and longer pedicle), and superficial-plane elevation reliably reduces bulk. Perforasome mapping similarly finds large territories for both patterns (~156-179 cm²) despite variation, with major perforators consistently present and occasional links toward the lateral circumflex femoral system.
Because thin/supra-fascial SCIP issues often come down to outflow, venous dye injection with clinical correlation identifies the SCIV as an independent, sizeable drainage network (≈2× the venae comitantes diameter) with communicating links and reports no higher flap loss or venous congestion when using SCIV-only drainage compared with venae comitantes or dual drainage.
Practical takeaway: cadaver injection evidence supports choosing the deep branch when size/pedicle length matter, elevating superficially for thinness, and planning robust venous outflow, often prioritising the SCIV.
Sources: (Sinna, 2010); (Zubler, 2021); (Gandolfi, 2020); (Sun, 2024)
Articles of the Week
3 Interesting Articles with One-Sentence Summaries
The SCIP flap reimagines the traditional groin flap by relying on a single perforator with just a 3-4 cm pedicle, allowing quicker elevation, primary thinning, minimal donor-site morbidity, and a concealed scar, all while preserving major vessels.
The original groin flap harnessed the superficial circumflex iliac vessels to create a reliable single-stage pedicled flap for hand and forearm resurfacing, offering a simpler, more versatile alternative to the traditional tube pedicle.
Every perforator supplies its own distinct vascular territory (perforasome) and adjacent perforasomes are connected through direct and indirect linking vessels, which reshaped the design and extending of perforator flaps in both pedicled and free tissue transfer.
