
In this week's edition
- ✍️ Letter from P'Fella
The community has spoken. Now we build. - 🖼️ Image of the Week
Rotation deformities in metacarpal fractures - 🚑 Technique Tip
Intra-articular base of thumb metacarpal fracture fixation - 📖 What Does the Evidence Say?
Metacarpal fractures: When is surgery actually worth it? - 🔥 Articles of the Week
Thumb base trauma & metacarpal fixes: 3 articles with 1-sentence summaries. - 💕 Feedback
Suggest ideas & give feedback!
A Letter from P'Fella
The Community Has Spoken. Now We Build.
And I’m really grateful for that, because it makes this feel like a community rather than a broadcast.
Across the last few questionnaires, we’ve had 100s of responses from 100s of people. I wouldn't want to label that as “engagement,” because I consider it a conversation. So instead of another letter where I just ask a question, I thought I’d share what came back and what we’re doing with it.
You Don’t Want “More Content”. You Want Usable Content.
This was probably the clearest pattern across all the responses.
When we asked what should be in an international curriculum, the top ask (by far) was step-by-step operative walkthroughs. Videos were close behind. After that came anatomy explained for operating, complication playbooks, acute algorithms, and checklists.
In other words, the things you actually reach for when you’re tired and the case is moving.
We also asked a follow-up: if you were building a core international plastics curriculum, what topics should sit at its centre? The responses were fairly consistent. Most clustered around the areas trainees repeatedly rotate through and rely on.
The theme is practical guidance. Essentially, "Don’t just tell me what it is. Show me how to do it, and what can go wrong."
You Want Quick Refreshers And The “What Catches You Out” Bits.
Most of you said the same thing: you want more insight into plastic surgery education, not more noise. And when we asked what you’d actually like more insight on, three things came up again and again.
- Most visited topics
- Super quick refreshers
- Most revisited complications & pitfalls
That’s a really honest reflection of how surgical learning actually works. It’s not always “sit down and study for two hours”. It’s “I’ve got five minutes, so remind me of the key decisions, and warn me what I’m about to miss.”
“International” Shouldn't Mean Generic.
The international curriculum responses came from 22 different locations. And the message wasn’t “add every topic under the sun.”
Instead, it was something more thoughtful: Make it portable, but real. Give the principles that travel across systems, but explain the differences that don’t.
So What Are We Doing With That?
We’re building an international curriculum that’s more than a library of articles. It’ll be structured around the things you keep asking for: step-by-step technique, decision-making, complications, and the “what to do next” parts that matter when you’re under time pressure.
The goal isn’t to make something generic. It’s to build a shared foundation that travels across training systems while still respecting that practice looks different depending on where you train and work.
Over the next few weeks, we’ll start showing you what this curriculum looks like as it takes shape: what’s in, what’s missing, and what we’re prioritising.
And we’ll continue doing this the same way we started: asking, listening, and feeding back what we build from what you tell us.
Genuinely, thank you for replying, for sharing what you actually need, and for being here each week.
With love,
P’Fella ❤️
Image of the Week
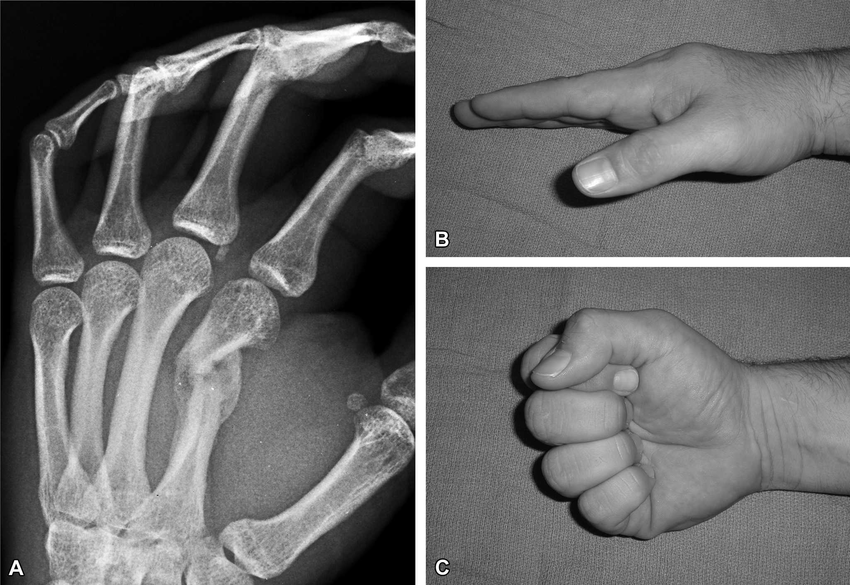
Rotation Deformities in Metacarpal Fractures
This image demonstrates an early malunion of a second metacarpal fracture (A) and the resulting rotational deformity seen clinically when the patient makes a fist (B-C).
Unlike angulation, even small degrees of rotation are poorly tolerated in the hand. When a metacarpal heals with rotational malalignment, the affected finger deviates from its normal trajectory, producing “scissoring” or overlap of the digits during flexion.
The key lesson is simple 👉 Rotation is a clinical diagnosis.
X-rays may underestimate the deformity, so the finger cascade during fist formation must always be assessed. Persistent malrotation is a common indication for reduction or fixation, as untreated rotational deformity leads to significant functional impairment.
Technique Tip
Intra-Articular Base of Thumb Metacarpal Fracture Fixation
This week's technique guide demonstrates operative fixation of an intra-articular fracture at the base of the thumb metacarpal, where the key principle is anatomic reduction of the joint surface to restore stability and reduce the risk of post-traumatic arthritis. These fractures are unstable because deforming forces from the thumb musculature tend to displace the metacarpal shaft, so surgery focuses on accurately reducing the articular fragment and maintaining that reduction with stable fixation.
The technical takeaway is that this is not just a “thumb fracture,” it is a joint reconstruction problem. Careful exposure, precise reduction of the articular surface, and appropriately contoured fixation are essential to preserve thumb CMC congruity and allow early motion while minimising long-term stiffness and degenerative change.
What Does the Evidence Say?
Metacarpal Fractures: When Is Surgery Actually Worth It?
When fixation is needed, the construct matters. In displaced fifth metacarpal neck fractures, antegrade intramedullary splinting produced better MCP joint motion, less shortening, less pain, and a better overall clinical score than retrograde crossed pinning, although grip strength and DASH scores were similar. In metacarpal shaft fractures requiring surgery, locking plates produced better range of motion, grip strength, rotational control, and DASH scores than intramedullary pinning, but at the cost of longer operative time and longer radiographic healing time.
Practical Takeaway: Treat uncomplicated fractures conservatively, but when you operate, prioritise fixation that controls rotation and permits early mobilisation for that specific fracture pattern.
Sources: (Wong, 2017); (Kollitz, 2014); (Schädel-Höpfner, 2007); (Dreyfuss, 2019)
Articles of the Week
3 Interesting Articles with One-Sentence Summaries
Stability of the thumb CMC joint hinges on the volar ulnar fragment anchored by the anterior oblique (beak) ligament, meaning Bennett fractures displace predictably and usually require fixation to restore joint congruity and preserve pinch strength.
For closed extra-articular metacarpal fractures, ORIF enables earlier mobilization without sacrificing overall outcomes, with a particular range-of-motion advantage in transverse shaft fractures, making fixation choice less about union and more about matching stability to rehabilitation demands.
Fasciculated intramedullary pinning provides enough stability to permit early mobilization while preserving motion and grip strength, making it a technically simple fixation strategy for displaced metacarpal neck fractures when conservative treatment is inadequate.
