
In this week's edition
- ✍️ Letter from P'Fella
Building a curriculum that actually travels - 🤓 The Sunday Quiz
Making some renovations! - 🖼️ Image of the Week
The intercostobrachial nerve during axillary dissection - 🚑 Technique Tip
Thoracodorsal to long thoracic nerve transfer - 📖 What Does the Evidence Say?
Axillary dissection in melanoma & cutaneous SCC: survival vs regional control - 🔥 Articles of the Week
High-risk cutaneous SCC, SLNB selection in cSCC, & cSCC and precursor lesion guidelines - 💕 Feedback
Suggest ideas & give feedback!
A Letter from P'Fella
Building a Curriculum That Actually Travels
Because plastic surgery isn’t practised in a vacuum. It’s practised inside systems with different referral pathways, different theatre times, different kits, different caseloads, different training structures, different cultural expectations, and different “normal”.
A registrar in London and a trainee in Kuala Lumpur might both be learning burns… but the system around burns can look completely different.
And yet, the patient still turns up with the same problem: a hand injury at 2am, a lower limb defect after trauma, a skin cancer that needs a plan, a burn that can spiral if the first decisions are wrong.
That’s the tension we’re trying to solve.
Not “one curriculum to replace everyone else’s”. More like a shared map. Something that’s useful wherever you work, and flexible enough to adapt to the reality you’re in.
What we mean by “international curriculum”
This isn’t about chasing a perfect syllabus. It’s about building a foundation that holds up across borders:
- Principles that don’t change: Anatomy, planning, reconstruction logic, wound healing, complications
- Decision-making that’s portable: “What’s the next safest step?”
- Technique with context: Why this flap, why this plane, what goes wrong, what to watch for
- Clear pathways for learners: So you’re not drowning in tabs
And yes, it includes articles. We already have a lot of those. But if we’re honest: a curriculum isn’t just a bunch of articles.
A curriculum is the stuff that actually helps you move from:
“I’ve heard of this” – “I can plan it” – “I can do it” – “I can teach it” – “I can fix things when it goes sideways.”
That requires more than text.
What we think we might be missing
If we’re going to do this properly, an international curriculum probably needs things like:
- Core “must-know” modules
- Step-by-step operative walkthroughs
- Decision trees/algorithms
- Complication playbooks
- Case-based learning
- Anatomy layers explained in surgical language
- Post-op protocols and common pitfalls
- Exam frameworks (where relevant), without making everything exam-brained
And I’m sure there are blind spots we can’t see from our side. So rather than guessing, I’d rather ask.
Help us build it
If we were to build a proper international curriculum, something you’d actually want to follow, what should be in it?
What do you wish existed when you started? What do you still find yourself looking up? What formats genuinely help you learn (or teach)?
We’ll read every response. And we’ll use it to shape what we build next.
With love,
P’Fella ❤️
The Sunday Quiz
Making Some Renovations!
Check back next week :)
Image of the Week
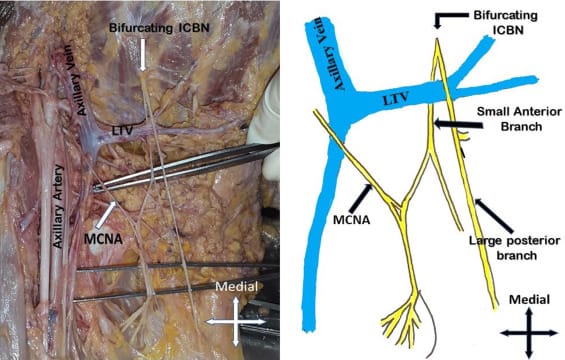
The Intercostobrachial Nerve During Axillary Dissection
This image highlights the intercostobrachial nerve (ICBN) during axillary dissection, shown here bifurcating near the axillary vein. A schematic alongside demonstrates its common branching pattern, including anterior and posterior divisions.
The ICBN (T2) provides sensory innervation to the medial upper arm and frequently crosses the operative field during nodal clearance. Its proximity to the axillary vein and lymphatic tissue makes it particularly vulnerable during Level I and II dissections for melanoma and SCC.
Preservation, when oncologically safe, reduces the risk of chronic paraesthesia, dysaesthesia, and neuropathic pain — a significant contributor to long-term morbidity after axillary surgery.
👉 Oncological clearance and functional preservation must coexist in the axilla.
Technique Tip
Thoracodorsal to Long Thoracic Nerve Transfer
Long thoracic nerve palsy leads to scapular winging and loss of forward elevation beyond 90° due to serratus anterior paralysis. This technique uses a distal posterior branch of the thoracodorsal nerve to reinnervate the distal long thoracic nerve via a lateral thoracic approach, targeting the portion of serratus anterior responsible for inferior angle stabilisation and scapular upward rotation.
Key principles are distal coaptation to shorten reinnervation time, preservation of adequate thoracodorsal input to maintain latissimus function, and tension-free microsurgical repair. In selected cases, this is combined with a proximal transfer (“double-level transfer”) to optimise serratus recovery and shoulder biomechanics.
What Does the Evidence Say?
Axillary Dissection in Melanoma & Cutaneous SCC: Survival vs Regional Control
For cutaneous SCC of the trunk/extremities, outcomes appear to track strongly with nodal status: presenting with regional nodal disease is a dominant adverse prognostic factor (remaining significant on multivariable analysis for recurrence/death risk). Histology matters too. Metastases cluster in thicker and poorly differentiated tumors, and certain subtypes are more aggressive. Perineural invasion is not “all equal”: larger-caliber PNI and the presence of additional high-risk features markedly increase the risk of nodal metastasis. Clinically extensive perineural spread also signals aggressive biology with poor outcomes despite intensive local therapy.
Sources: (Faries, 2017); (Mullen, 2006); (Petter & Haustein, 2000); (Carter, 2013); (McNab, 1997)
Articles of the Week
3 Interesting Articles with One-Sentence Summaries
In high-risk cutaneous SCC, tumour thickness >4 mm and recurrence predict early metastasis more reliably than sentinel lymph node biopsy, shifting the surgical priority from nodal sampling to vigilant 2-year surveillance.
Sentinel node positivity concentrates in AJCC T2 tumours >2 cm and, more precisely, in the alternative system’s T2b category, positioning tumour stage as the operative criterion for considering SLNB.
These guidelines reposition cutaneous SCC management around formal risk stratification, defining surgical margins, indications for Mohs, adjuvant therapy, and follow-up intensity according to tumour biology rather than size alone.
