
In this week's edition
- ✍️ Letter from P'Fella
3 Lessons from London - 🤓 The Sunday Quiz
How well do you know flexor tendon injuries? - 🖼️ Image of the Week
Cadaveric example of a vascularised tendon graft. - 🚑 Technique Tip
EIP vascularised tendon graft. - 📖 What Does the Evidence Say
Is Pulvertaft weave the best option? - 🔥 Articles of the Week
Tendon defects, transfers, & hamstring tendons: With 1-sentence summaries. - 💕 Feedback
Suggest ideas & give feedback!
A Letter from P'Fella
3 Lessons from London
Ideas everywhere, teams sprinting to build something real, and some genuinely impressive projects (shout out to Claribone).
But what stuck with me most weren’t the projects—it was the lessons. A hackathon compresses months of work into hours, and you see people’s instincts play out in real time. Here are three things I took away:
1. Keep it focused: A lot of teams went broad, trying to solve everything at once. The best ideas were the simplest—tackling one problem, for one clear customer.
2. Stop overthinking: Plenty of groups got stuck planning. The winning teams just started building. They tested, failed, fixed, and by the end of the weekend had something real in their hands.
3. Show, don’t tell: A working prototype always beats a polished pitch. Even a rough demo carries more weight than slides or words.
It made me wonder: what if we applied this to education in plastic surgery? Instead of endless debates about curriculum, imagine focused sprints where we just build the tools trainees actually need.
Sometimes progress isn’t about having the smartest idea—it’s about starting small, keeping it sharp, and just doing the work.
It got me thinking....
With love,
P’Fella ❤️
The Sunday Quiz
How Well Do You Know Flexor Tendon Injuries?
Join The Weekly Quiz in each edition of thePlasticsPaper. This is the final round of seven rounds!
The top scorer wins one of the first print Foundations at a discount!
Image of the Week
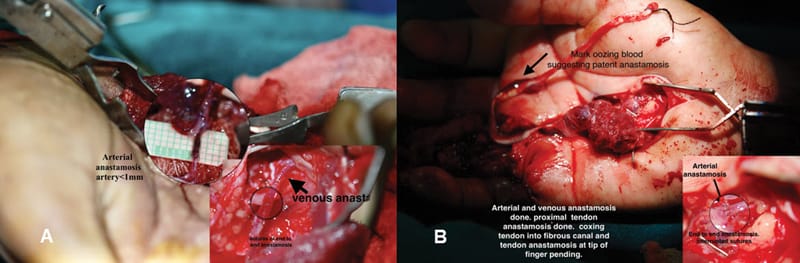
Cadaveric Example of a Vascularised Tendon Graft
This week’s image shows a cadaveric demonstration of a vascularised tendon graft, highlighting both arterial and venous anastomoses. These grafts are valuable in complex tendon reconstruction, particularly when both structural and biological support is needed to optimise healing.
The image shows the completed vascular connections and the preparation of the tendon within the fibrous canal. Vascularised tendon grafts are increasingly relevant in secondary reconstruction where the tendon bed is scarred or poorly vascularised, such as in chronic injuries or post-infection settings.
Keep an eye out for the inset detail showing <1 mm anastomoses; a reminder of the precision and microsurgical finesse required.
Technique Tip
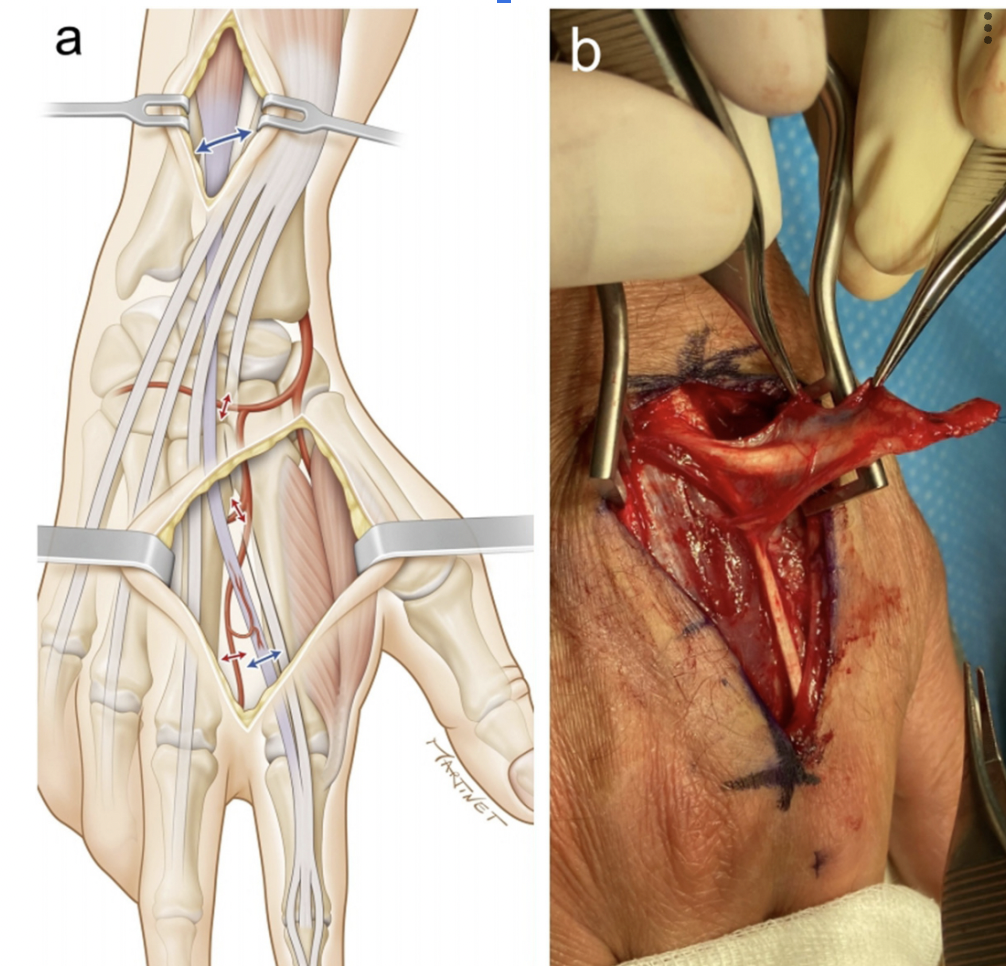
EIP Vascularised Tendon Graft
This week’s tip focuses on a fundamental but critical move during dorsal hand approaches: safe and strategic extensor tendon retraction.
In both the diagram and intra-op image shown, you’ll notice the use of Senn retractors and mosquito clips to protect and mobilize the extensor tendons. Careful retraction improves access to the underlying structures (e.g., metacarpals, joints, plates) while preserving tendon integrity.
Tip: Retract longitudinally, not laterally, while avoiding excessive tension to reduce the risk of tendon fraying or delayed repair issues.
This technique is especially relevant when working around dorsal plates, midshaft fractures, or when exposing intrinsic muscles for reconstruction.
What Does the Evidence Say?
Is Pulvertaft Weave the Best Option?
Van Royen et al. (2021) demonstrated that a modified core suture Pulvertaft weave using FiberLoop 4.0 showed significantly superior biomechanical properties compared to the traditional technique, with 5 times greater strength in stiffness, first failure load, and ultimate failure load. Crook et al. (2013) introduced a novel loop weave that demonstrated significantly higher initial failure and ultimate strengths compared to the Pulvertaft weave, with failures occurring through tendon splitting rather than suture failure. Duprat et al. (2017) found no significant difference in failure load between Pulvertaft weave and step-cut suture techniques (116N vs 103N), though step-cut repairs had smaller cross-sectional areas. Bidic et al. (2009) showed that lasso repairs achieved equivalent maximum load to Pulvertaft weaves (155.8N vs 159.7N) while requiring less weave time and tendon length.
Articles of the Week
3 Interesting Articles with One-Sentence Summaries
Single-stage vascularized FDS tendon transfers based on the ulnar vessels achieved ~178° total active motion with fewer complications than staged grafting, offering a viable alternative in select cases.
For Sunderland IV-V injuries, tendon and nerve transfers are often used together, nerve transfers being increasingly popular for excellent outcomes, and tendon transfers being a reliable backup if nerve recovery fails.
Cadaveric analysis shows the gracilis tendon matches flexor tendon dimensions for staged reconstruction (except in the little finger), while the semitendinosus is too thick for use in intact pulley systems.
