

Summary Card
Overview
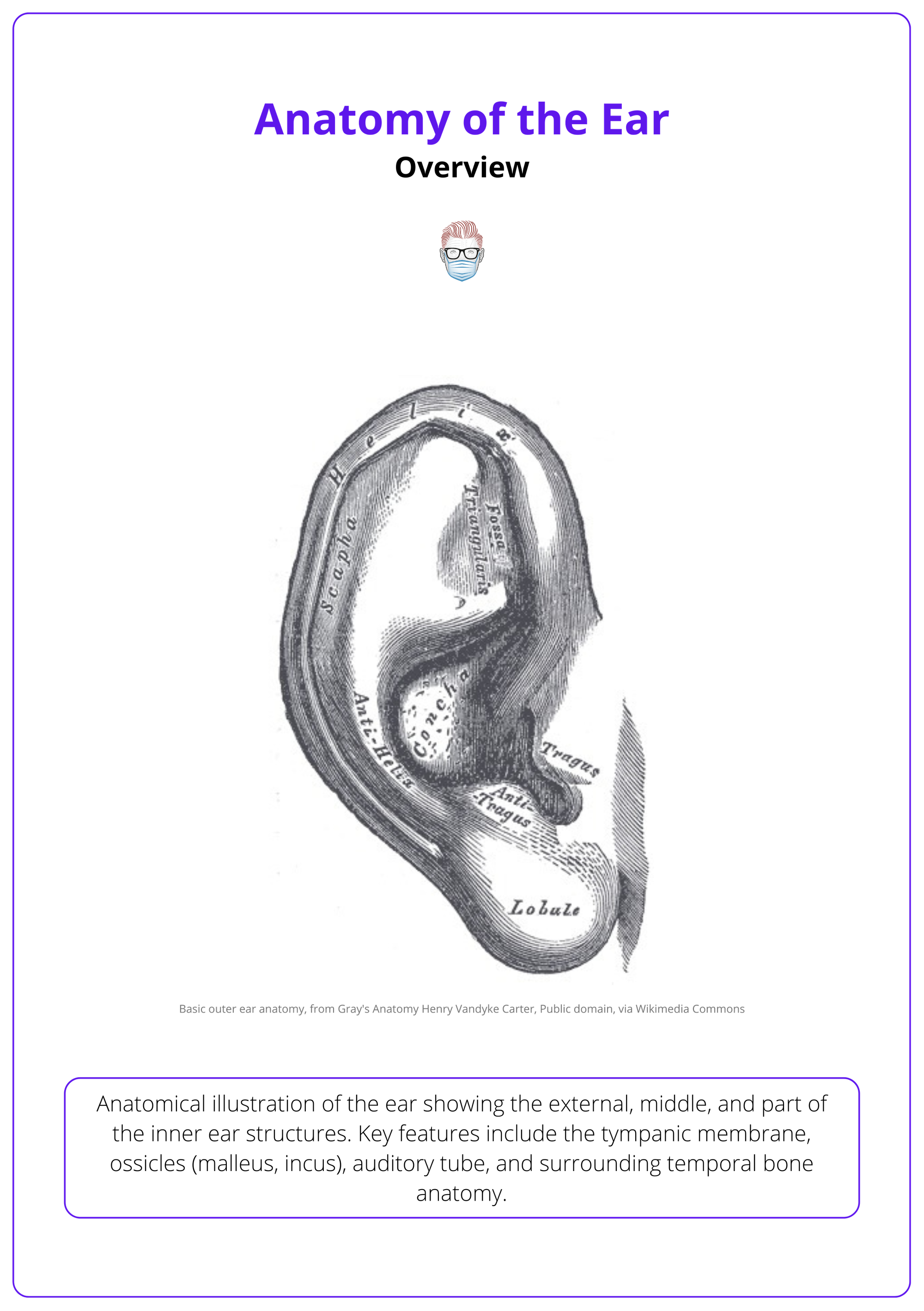
The external ear is a specialised composite structure composed of cartilage, skin, and soft tissue. It plays vital roles in hearing, facial aesthetics, and protecting the auditory system.
Neurovascular Supply
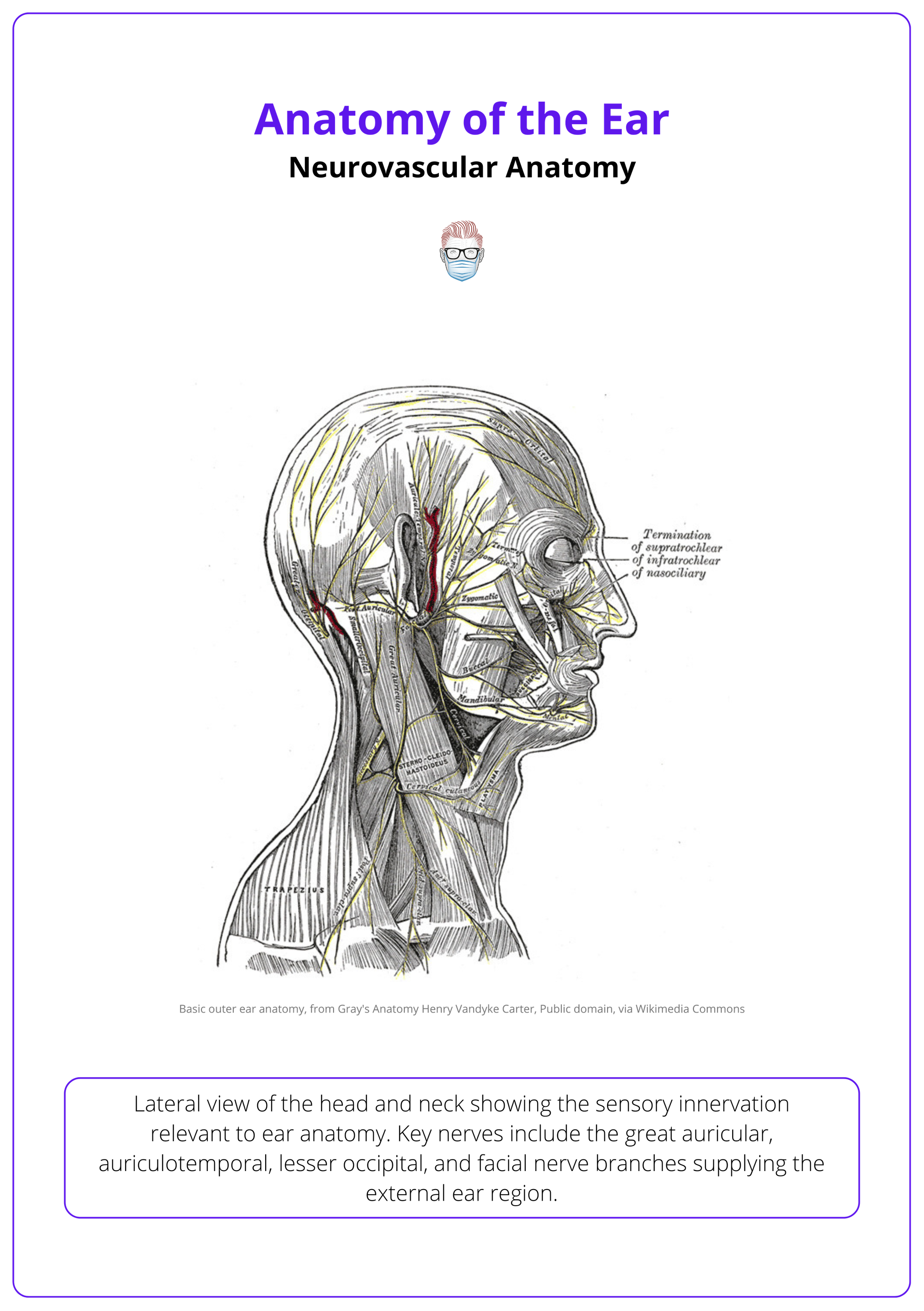
The ear receives a complex neurovascular supply derived from cranial nerves, cervical plexus branches, and the external carotid artery system.
Anatomical Landmarks
The auricle (pinna) has distinct anatomical substructures that assist in sound conduction and serve as critical reference points in clinical and surgical settings.
Aesthetic Subunits
Dividing the auricle into aesthetic subunits improves surgical planning and ensures natural and harmonious reconstruction.
Auricular Muscles
The auricle contains vestigial striated muscles innervated by the facial nerve, with minimal functional role in most individuals.
External Auditory Canal
The external auditory canal is a 25 mm S-shaped passageway that directs sound waves to the tympanic membrane. It comprises cartilaginous and osseous segments and is lined with skin containing ceruminous glands.
Primary Contributor: Dr Mustafa Qais Al-Khafaji.
Verified by thePlasticsFella ✅
Overview of Ear Anatomy
The external ear is a specialised composite structure composed of cartilage, skin, and soft tissue. It plays vital roles in hearing, facial aesthetics, and protecting the auditory system.
The external ear (auricle) is a specialised structure essential for sound conduction, aesthetic contouring, and surgical reference — composed of elastic cartilage, skin, and soft tissue.
Structural Composition
- Elastic cartilaginous framework provides shape and flexibility.
- Covered by tightly adherent skin, especially on the anterior surface.
- Contains ceruminous and sebaceous glands, neurovascular bundles, and vestigial muscles.
Functional Roles
- Directs sound waves into the external auditory canal, enhancing auditory localization.
- Contributes to facial symmetry and contour, particularly relevant in aesthetic and reconstructive surgery.
- Acts as a surgical landmark due to its predictable anatomy and topography.
Clinical Importance
- Serves as a guide in reconstructive surgery, especially for,
- Auricular defects
- Microtia repair
- Otoplasty
- Used to assess cutaneous malignancies (e.g., BCC, SCC) due to sun-exposed position.
- Involved in nerve distribution zones, relevant for regional blocks and flap planning.
- The Arnold Reflex (via vagus nerve) may trigger cough or nausea during otologic exams.
The image below illustrates the ear and its external and middle structures.
The auricle continues to grow throughout life, primarily due to cartilage elasticity and gravitational pull, hence the common “droopy ear” appearance in elderly patients (Heathcote, 1995).
Neurovascular Supply of the Ear
The ear receives a complex neurovascular supply derived from cranial nerves, cervical plexus branches, and the external carotid artery system.
The external ear receives a complex neurovascular supply critical for its function, sensory innervation, and safe surgical manipulation. Understanding this anatomy is essential in trauma repair, local flap design, and regional anesthesia.
Motor Innervation
- Temporal branch of the facial nerve (CN VII) innervates the auricular muscles.
- These striated muscles (anterior, superior, and posterior auricular) are vestigial in humans, with minimal voluntary movement in most individuals.
- During flap elevation or cartilage scoring, preserving these nerve branches minimizes postoperative distortion or synkinesis.
Sensory Innervation
The auricle’s sensory innervation is richly sourced from cranial and cervical nerves.
- Auriculotemporal Nerve (branch of CN V3): Anterior auricle and anterior canal walls.
- Great Auricular Nerve (C2, C3): Lower posterior auricle.
- Lesser Occipital Nerve (C2): Upper posterior auricle.
- Auricular Branch of the Vagus Nerve (Arnold’s Nerve) (CN X): Posterior canal wall.
- Facial Nerve (CN VII): Contributes to canal innervation via communication with CN X.
Key nerves regarding ear anatomy are illustrated below.
Glands & Secretions
Glandular structures in the external ear serve a protective and lubricating role, especially within the auditory canal.
- Ceruminous glands
- Modified apocrine sweat glands located in the cartilaginous portion of the external auditory canal.
- Secrete cerumen (earwax) — a mixture of cerumen, sebum, and desquamated keratinocytes.
- Functions: Antimicrobial barrier, moisture regulation, and protection against foreign bodies.
- Sebaceous glands
- Found adjacent to ceruminous glands.
- Contribute sebum, enhancing lubrication and preventing canal dryness.
Arterial Supply
The external ear is supplied predominantly by branches of the external carotid artery, ensuring perfusion for tissue viability and surgical flaps.
- Posterior Auricular Artery: Supplies the posterior auricle and lobule.
- Superficial Temporal Artery: Provides anterior and superior auricular supply.
- Maxillary Artery: Minor branches contribute, particularly to the deep auricular canal.
These vessels are often involved in postauricular flaps, composite grafts, and helical rim reconstructions. Preserving arterial branches reduces the risk of flap necrosis.
Venous Drainage
- Mirrors the arterial supply, with drainage into the external jugular venous system via,
- Pterygoid venous plexus
- Maxillary vein
- This pathway is clinically relevant in facial infections that may retrogradely spread via valveless connections.
Blood supply to the ear is derived from the external carotid artery system. Drainage and lymphatic routes are clinically important for infection and malignancy spread.
Lymphatic Drainage
Lymphatic drainage routes are essential in the spread of infections and cutaneous malignancies. This includes preauricular nodes, mastoid (postauricular) nodes, and superficial cervical lymph nodes.
The lymphatic drainage of the auricle follows a predictable pattern, with each node group responsible for specific regions. This is summarised below.
Lymphatic drainage of the head and neck is illustrated below.

Complete auricular anesthesia requires blocking the auriculotemporal (V3), great auricular (C2–C3), and lesser occipital (C2) nerves. Each supplies a distinct zone of the auricle: anterior, lower/posterior, and upper/posterior respectively. This triple block is ideal for procedures like otoplasty, trauma repair, and skin excisions, providing broad sensory coverage with local anesthesia.
Anatomical Landmarks of the Ear
The auricle (pinna) has distinct anatomical substructures that assist in sound conduction and serve as critical reference points in clinical and surgical settings.
The auricle (pinna) constitutes the visible portion of the external ear. Structurally, it is composed of a cartilaginous framework covered by tightly adherent skin and delineated by anatomically distinct elevations and depressions. These features function to collect and direct sound toward the external auditory canal and serve as critical references in surgical reconstruction, trauma repair, and oncologic excision.
Principal Landmarks
- Helix: The outermost convex margin of the auricle, originating superior to the external auditory canal and arching posteriorly along the lateral ear.
- Cauda Helicis: The inferior terminal portion of the helix, merging with the lobule.
- Antihelix: An inner, C-shaped cartilaginous ridge anterior and parallel to the helix. It bifurcates into,
- Crus Superior and Crus Inferior: Superior and inferior limbs enclosing the fossa triangularis.
- Fossa Triangularis: A triangular concavity located between the two crura of the antihelix.
- Scapha: A longitudinal groove situated between the helix and antihelix.
- Tragus: A prominent cartilaginous projection situated anterior to the external auditory meatus; functions in partially occluding the canal.
- Antitragus: A cartilaginous eminence located inferior to the antihelix and opposite the tragus.
- Concha: The central, concave depression leading directly into the external auditory canal. It is subdivided into:
- Cymba Conchae: The superior component.
- Cavum Conchae: The inferior component adjacent to the canal entrance.
- Lobule: The soft, inferior portion of the auricle lacking cartilage; composed primarily of adipose and fibrous tissue.
Supplementary Landmarks
- Auricular Tubercle (Darwin’s tubercle): A vestigial prominence occasionally observed along the posterior helix—an evolutionary remnant.
- Spine of Helix: A subtle protuberance located near the caudal curvature of the helix.
- External Auditory Meatus: The aperture of the external auditory canal leading to the tympanic membrane.
- Preauricular Region: An anatomically significant area anterior to the tragus, commonly implicated in congenital anomalies (e.g., preauricular pits), infections, and neoplastic processes.
The auricular tubercle (Darwin’s tubercle) is a small cartilaginous projection found on the posterior aspect of the helix in approximately 10% of the population. It is considered a vestigial trait linked to ancestral mobility of the ear.
Aesthetic Subunits of the Auricle
Dividing the auricle into aesthetic subunits improves surgical planning and ensures natural and harmonious reconstruction.
The auricle can be conceptualized into distinct aesthetic subunits based on its natural topography. This subunit-based approach is especially helpful in reconstructive and aesthetic surgery, allowing for the restoration of form and contour with minimal distortion.
Commonly Recognised Aesthetic Subunits
Each subunit and their components are summarised below.
- Helical Rim: The outer margin of the ear, from the root to cauda helicis.
- Antihelix Complex: Includes the antihelix and its crura, and the triangular fossa.
- Conchal Bowl: The cymba and cavum conchae, forming the central depression.
- Tragus/Antitragus Unit: The paired anterior projections flanking the concha.
- Lobule: The inferior, non-cartilaginous portion of the auricle.
Surgeons may also consider adjacent zones, such as the preauricular skin and mastoid region, when designing flaps or incisions to maintain contour and conceal scars.
When reconstructing auricular defects (e.g., after trauma or tumour excision), try to replace lost tissue with matching contour, texture, and thickness from the same aesthetic unit.
Muscles of the Auricle
The auricle contains vestigial striated muscles innervated by the facial nerve, with minimal functional role in most individuals.
The auricle is connected to the surrounding soft tissues and the scalp by several small striated muscles. These are generally rudimentary in humans and have limited voluntary function.
Auricular muscles, their location, and function are summarised below.
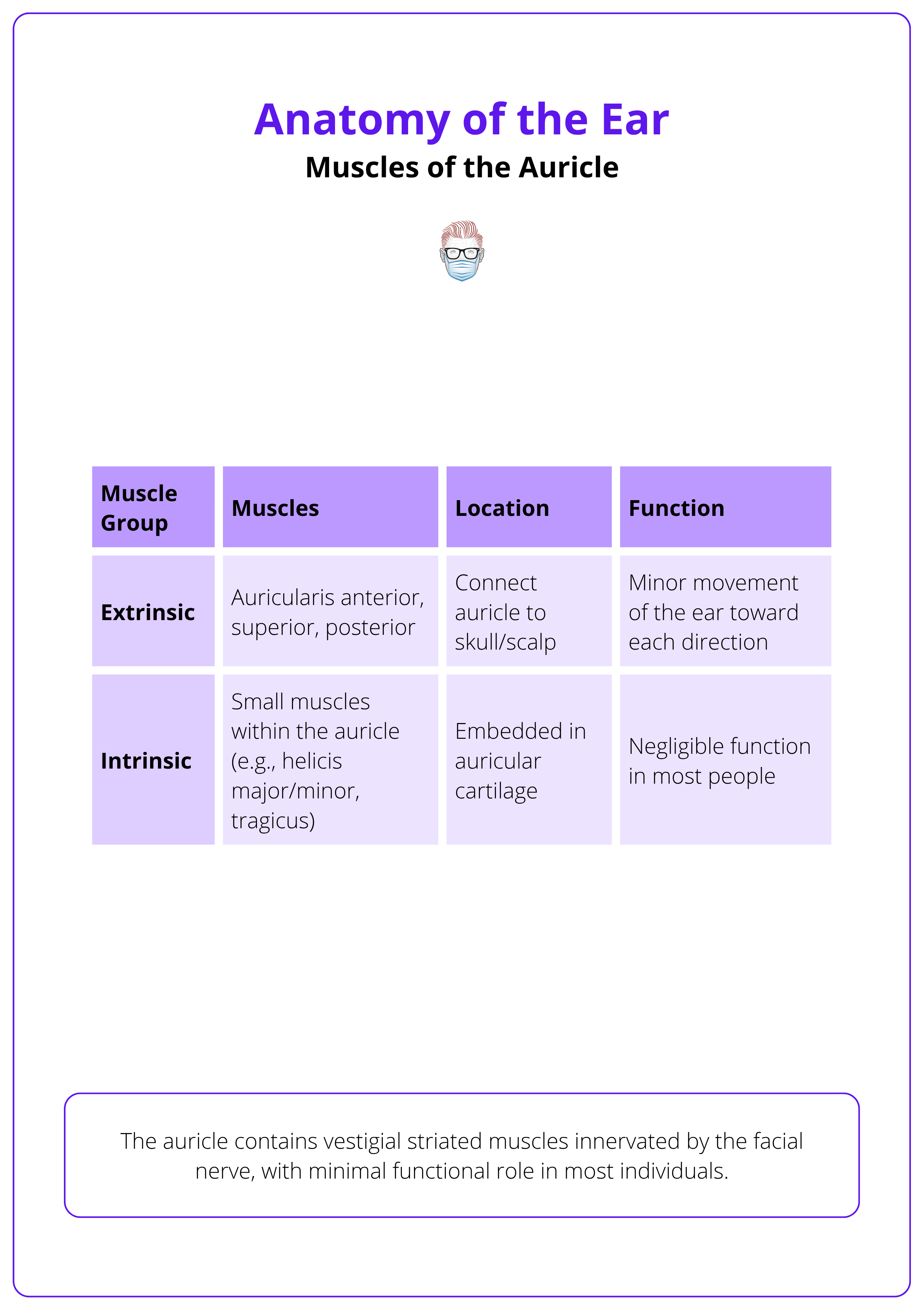
- All auricular muscles are innervated by the temporal branch of the facial nerve (CN VII).
- In most individuals, these muscles are underdeveloped and non-functional.
- Some people can voluntarily move their ears using these muscles — a trait with no known clinical significance but notable for its rarity.
Although functionally insignificant, the presence and location of these muscles must be considered during flap elevation or cartilage scoring to avoid unintended injury.
External Auditory Canal
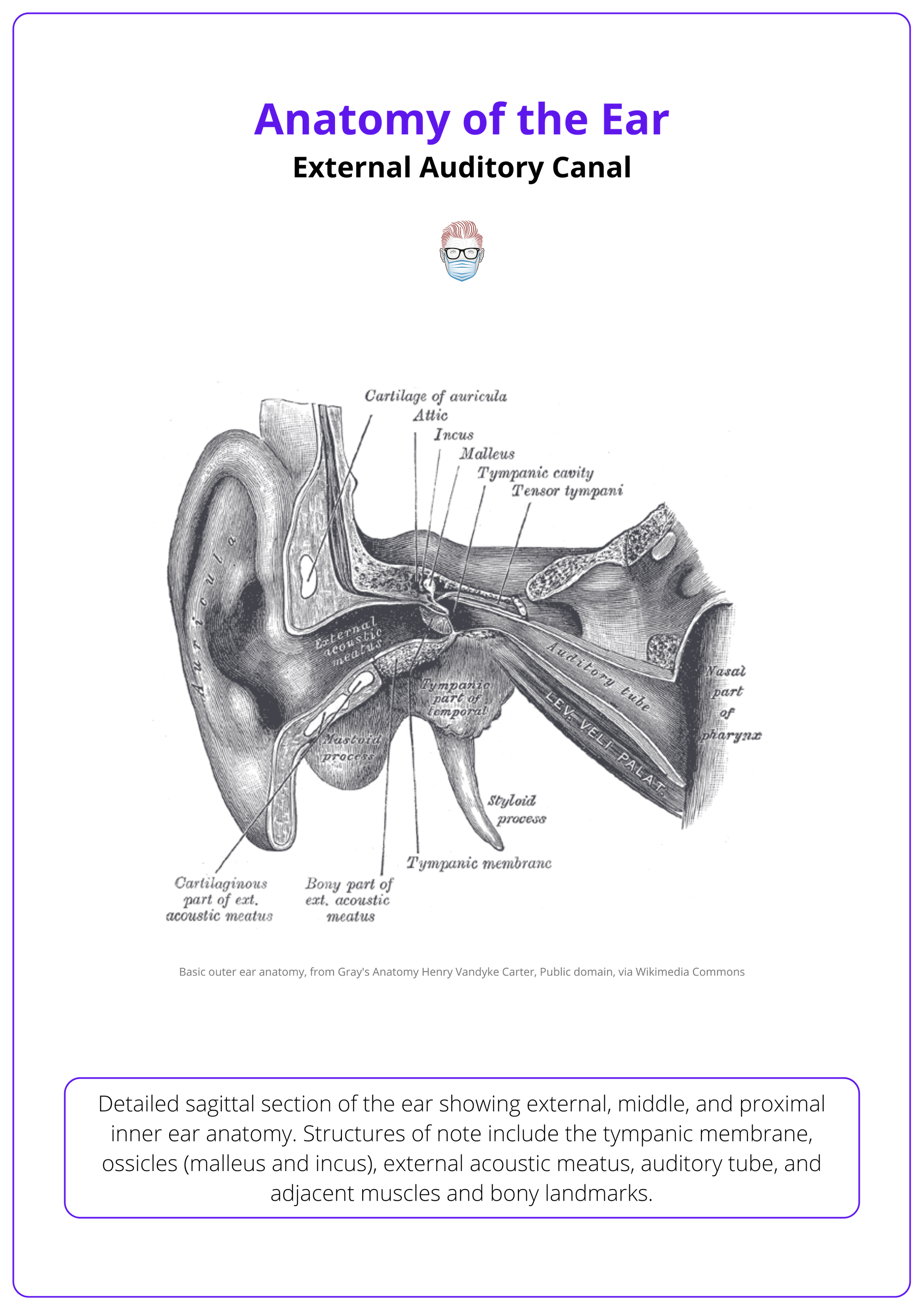
The external auditory canal is a 25 mm S-shaped passageway that directs sound waves to the tympanic membrane. It comprises cartilaginous and osseous segments and is lined with skin containing ceruminous glands.
The external auditory canal, or the external acoustic meatus, serves as the conduit between the auricle and the tympanic membrane. It plays a vital role in sound conduction and the protection of the middle and inner ear.
Anatomy and Structure
- Length: ~25 mm (2.5 cm) in adults.
- Shape: S-shaped, curving anteriorly then posteriorly.
- Subdivisions
- Outer third (≈8–10 mm)
- Composed of elastic cartilage.
- Mobile, with hair follicles, sebaceous and ceruminous glands.
- Inner two-thirds (≈15–17 mm)
- Composed of bone (tympanic part of temporal bone).
- Fixed and narrower.
- Lined by thin skin tightly adherent to the periosteum.
- Outer third (≈8–10 mm)
The image below illustrates the external auditory canal.
During otoscopy, the auricle is gently pulled upward and backward to straighten the S-curve and allow clear visualization of the tympanic membrane.
Conclusion
1. Overview: The external ear is a complex structure of cartilage, skin, and soft tissue that aids hearing and facial aesthetics. Anatomical knowledge is essential for reconstructive, congenital, and trauma-related procedures.
2. Neurovascular Anatomy: The auricle is innervated by cranial and cervical nerves and vascularised by branches of the external carotid. Ceruminous glands produce protective earwax, and vagal stimulation may trigger the Arnold reflex.
3. Auricular Landmarks: The auricle features distinct ridges and depressions (e.g. helix, concha, tragus) that direct sound and guide surgical reconstruction. Each substructure has clinical and aesthetic relevance.
4. Aesthetic Subunits: Dividing the ear into aesthetic zones such as the helical rim, conchal bowl, and lobule, guides reconstruction to restore natural form and conceal scars effectively.
5. Auricular Muscles: The ear contains vestigial intrinsic and extrinsic muscles, innervated by CN VII. Though functionally minimal, they should be preserved during surgery to avoid tissue distortion.
6. External Auditory Canal: The 25 mm S-shaped auditory canal transmits sound to the tympanic membrane. Its outer third is cartilaginous with glands, and the inner two-thirds are bony and fixed.
Further Reading
- White HJ, Helwany M, Biknevicius AR, Peterson DC. Anatomy, head and neck, ear organ of Corti. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; January 14, 2023.
- Altafulla J, Iwanaga J, Lachkar S, et al. The great auricular nerve: anatomical study with application to nerve grafting procedures. World Neurosurg. 2019;125:e403-e407.
- Young AS, Rosengren SM, Welgampola MS. Disorders of the inner-ear balance organs and their pathways. Handb Clin Neurol. 2018;159:385-401.
- Hohman MH, Jamal Z, Krogmann RJ, King KC. Auricular hematoma. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; May 1, 2024.
- Szmuilowicz J, Young R. Infections of the ear. Emerg Med Clin North Am. 2019;37(1):1-9.
- Osborn HA, Goldsmith TA, Varvares MA. Assessing functional outcomes in head and neck surgical oncology. Head Neck. 2019;41(7):2051-2057.
- Markkanen S, Niemi P, Rautiainen M, et al. Craniofacial and occlusal development in 2.5-year-old children with obstructive sleep apnoea syndrome. Eur J Orthod. 2019;41(3):316-321.
- Birgfeld C, Heike C. Craniofacial microsomia. Clin Plast Surg. 2019;46(2):207-221.
- Szymanski A, Geiger Z. Anatomy, Head and Neck, Ear. [Updated 2023 Jul 24]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470359/
