

Summary Card
Definition of Syndactyly
A failure of differentiation fuses soft tissue ± bone of the finger
Classification of Syndactyly
This can be classified as incomplete or complex, simple or complex.
Diagnosis of Syndactyly
A clinical diagnosis. Bony involvement is confirmed on the X-Ray.
Management of Syndactyly
Before the age of 2. Earlier if length discrepancy or border digits.
Definition of Syndactyly
Syndactyly is a congenital hand malformation defined as a "failure of differentiation" by Swanson or a "malformation of unspecific axis" according to OMT classification.
It can be classified as simple (soft tissue), complex (soft tissue and bone), complete (fusion of adjacent nails), or incomplete.
The image below illustrates a case of Syndactyly.
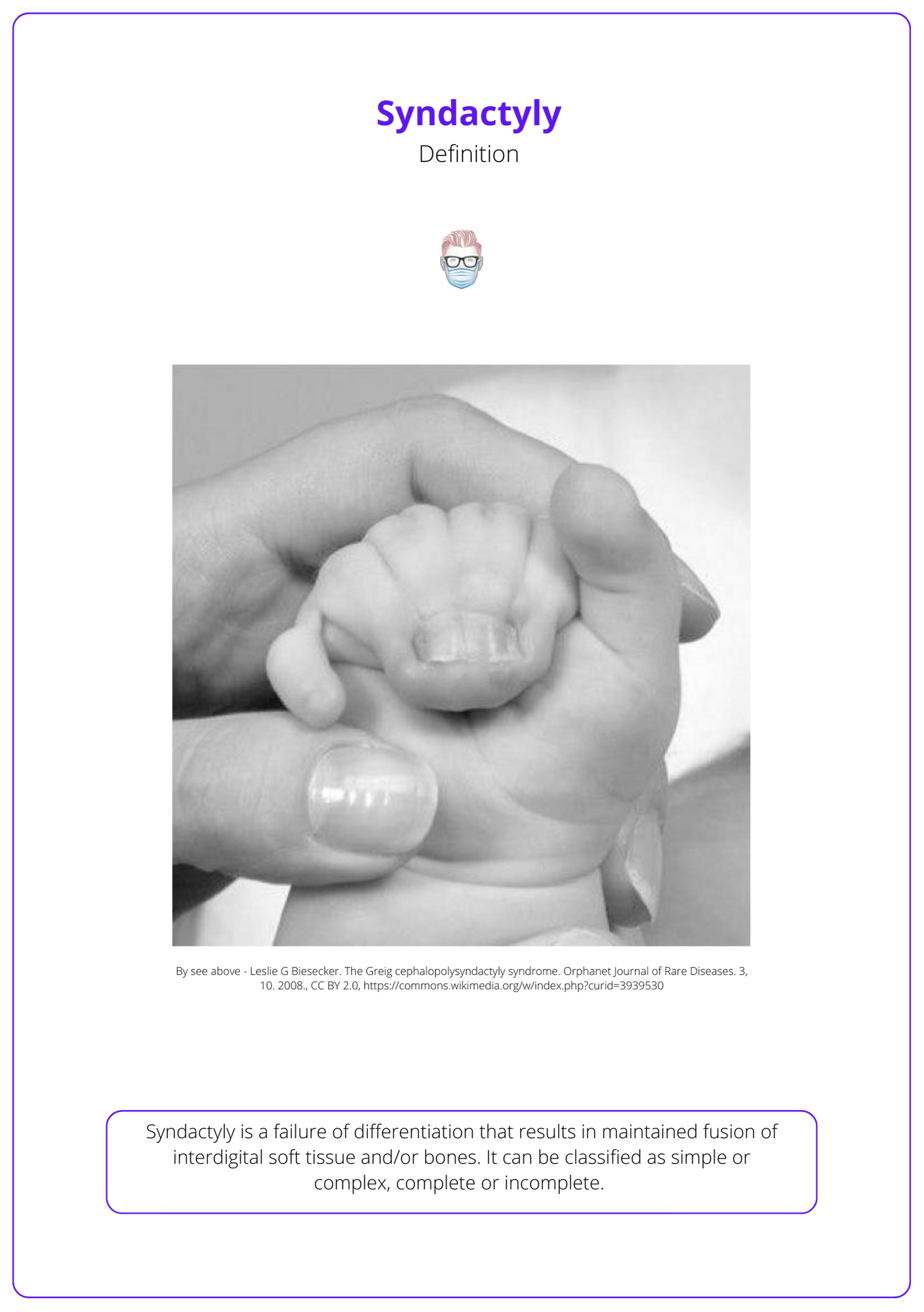
A failure in apoptosis results in the fusion of interdigital soft tissue and bones during weeks 6-8 of gestation. This is the result of activation, suppression, and overexpression.
- WNT is activated.
- BMP and Retinoic acid suppression.
- FGF-8 is overexpressed in the AER.
Classification of Syndactyly
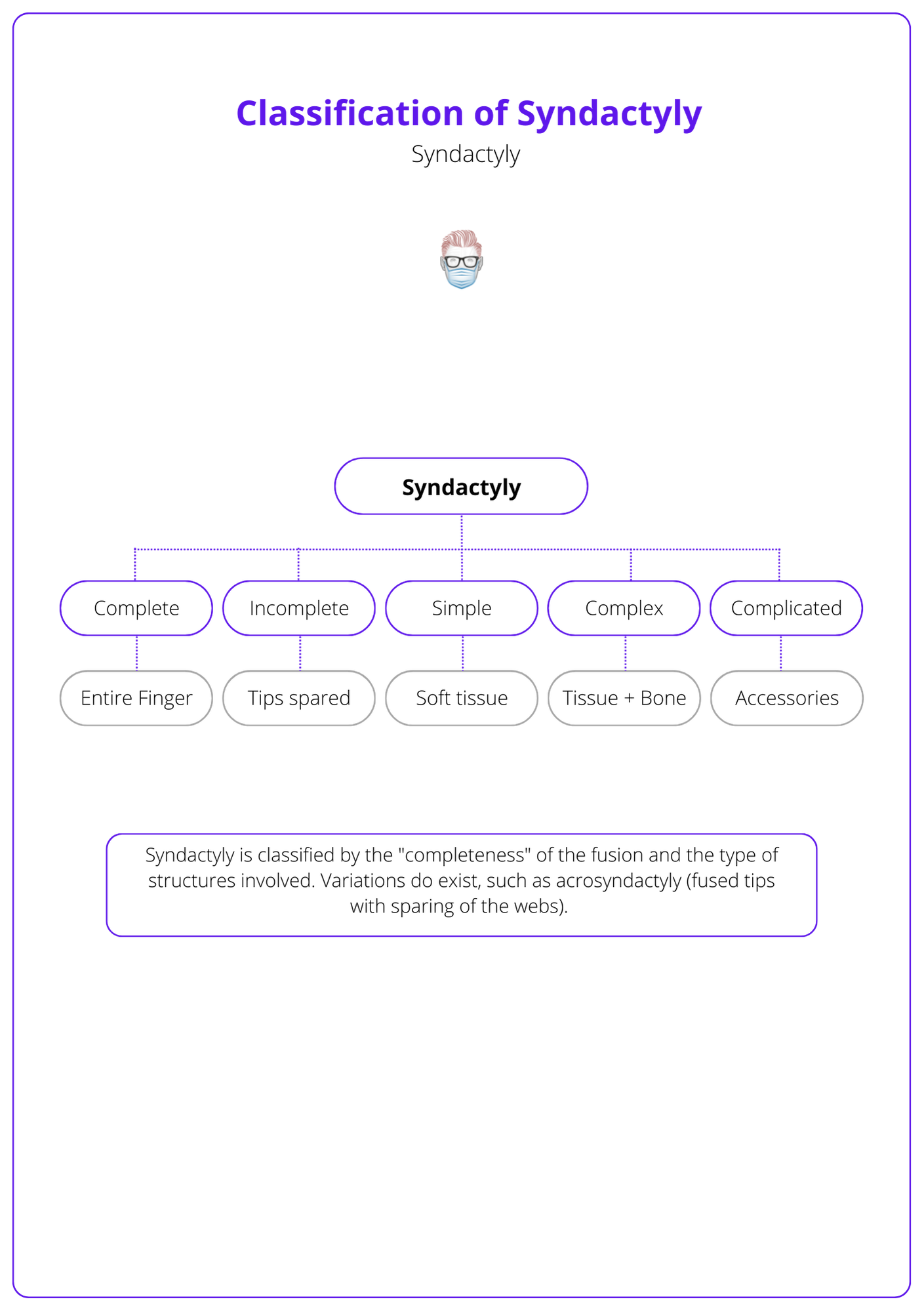
Syndactyly is classified as complete or incomplete, simple or complex. This is related to the extent of fusion and structures involved.
Syndactyly is classified by the extent of the fusion (entire finger or partial) and the structures (bone or soft tissue) involved.
- Simple: no synostosis (soft tissue only).
- Incomplete: fusion does not involve distal phalanx or overlying soft tissue.
- Complete: fusion involves the distal phalanx and/or overlying soft tissue.
- Complex: soft tissue with adjacent phalangeal fusion (synostosis).
- Complicated: accessory digits or phalanges, additional cleft hand.
- Acrosyndactyly: shortened digits fused distally with proximal fenestration.
This classification is illustrated in the diagram below.
Several phenotypic subtypes can result in synopolydactyly, a fusion of border digits, and even polydactyly of all digits.
Diagnosis of Syndactyly
Syndactyly is a clinical diagnosis that can occur in isolation or with an association syndrome. A plain X-ray will confirm synostosis.
Clinical Findings
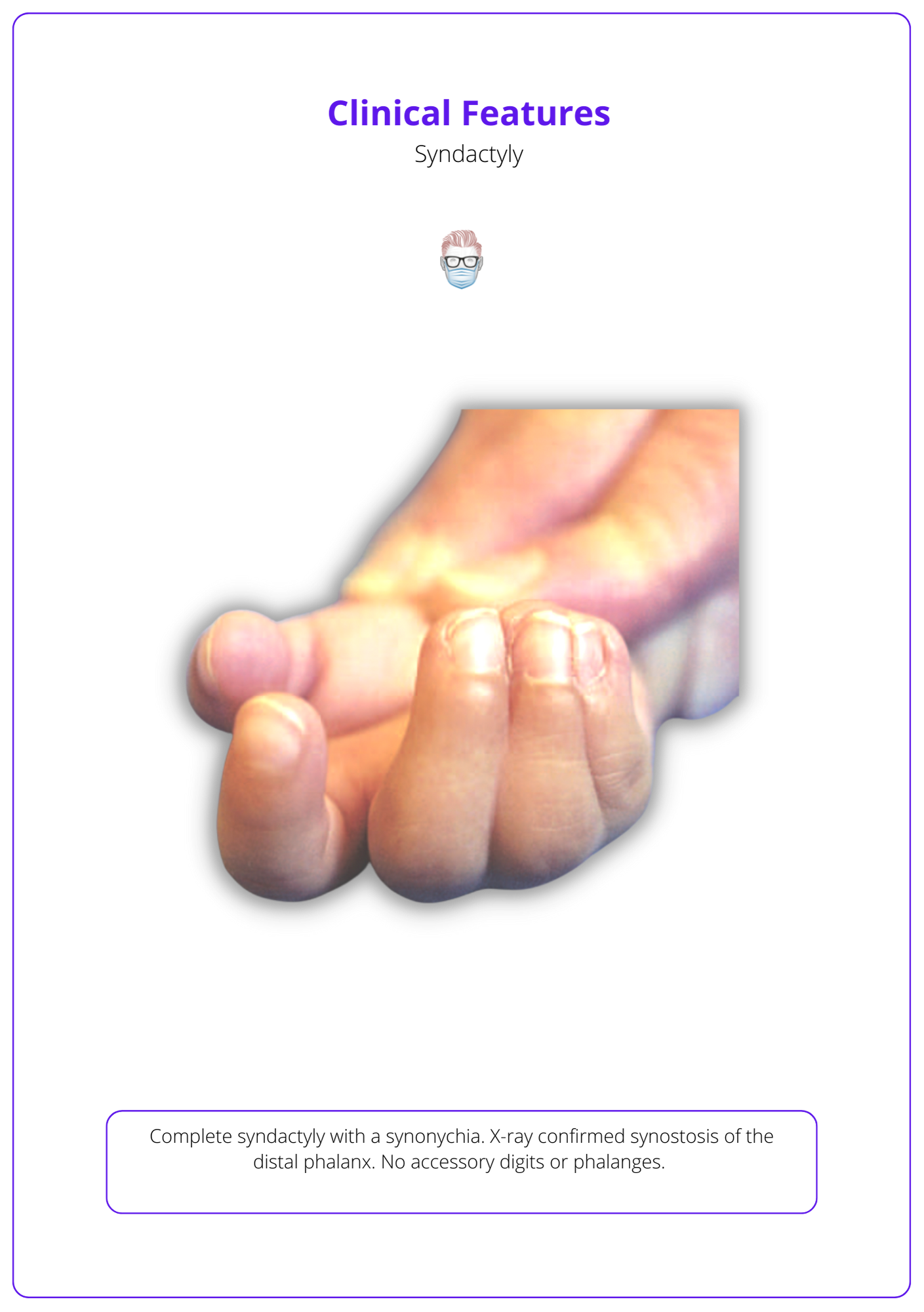
Syndactyly is a clinical diagnosis. It most commonly occurs in the middle-ring fingers and can be associated with other structural abnormalities.
It typically occurs in caucasian males with a family history and can be bilateral in ~50% of cases.
The below image illustrates the clinical features of Syndactyly.
The important pathological features of Syndactyly include:
- Bone: degrees of synostosis, joints usually preserved unless symphalangism.
- Ligaments: Cleland's and Grayson's ligaments thickened and coalesced.
- Tendons: duplicated or shared flexor and extensor tendons and sheaths.
- Neurovascular: duplicate or shared vessels and nerves.
- Skin: short of skin.
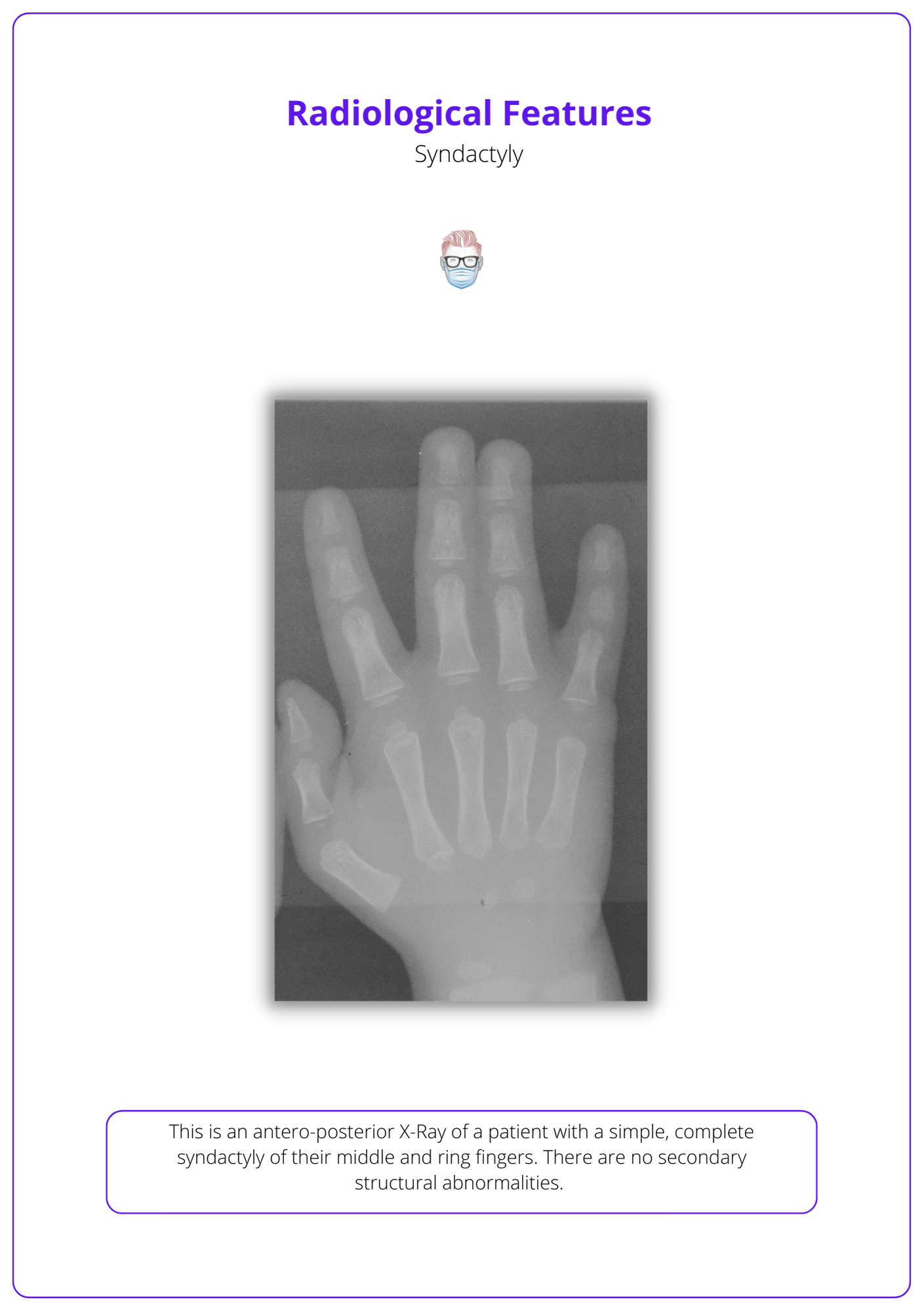
Radiological Findings
Check the image below for the radiological features of Syndactyly.
Associated Features
Syndactyly can be associated with other structural and craniofacial conditions including,
- Poland Syndrome: chest wall abnormalities and symbrachydactyly.
- Apert Syndrome: craniosynostosis and complex, bilateral syndactyly with symphalangism.
- Carpenter syndrome.
- Acrocephalopolysyndactyly
- Constriction ring syndrome (distal digital fusion, proximal digit fenestrations).
- Familial syndactyly is associated with syndactyly of the second and third toes.
- Timothy Syndrome: long Q-T can lead to sudden cardiac arrest.
Management of Syndactyly
Syndactyly is generally treated in the first 24 months. This is influenced by the finger(s), webspace, and length discrepancies.
Patient care for Syndactyly should be individualised. In the immediate setting, patient education and family counselling are essential. This should all be managed by a multi-disciplinary team.
Timing of surgery
Syndactyly release should be performed by after the age of 1 and ideally before age 2. The exact timing is influenced by the type of finger and webspace involvement.
- Earlier surgery if border digits are involved or a length discrepancy (~6 months).
- Later surgery if "similar" digits are involved (e.g. ring-long, long-index) as a larger hand enables a technically more straightforward operation with more predictable results.
Principles of Surgery Techniques
Surgery aims to separate digits, create minimal scarring, and respect the web space. This is performed through a combination of flaps and grafts adhering to the following principles:
Timings
- Age: between 1-2 years or ~6 months if fusion of unequal digits.
- Length: release digits with length discrepancy first.
- Location: release border digits first (ring-little, thumb-index).
- Multiple digits: staged release to avoid vascular issues ~3-6 months apart.
- Bilateral: simultaneously if < 18 months (less active) or staged if older.
Technique
- Incisions: dorsal and volar interdigitating zigzag 60° flaps to the midline whilst preserving the paratenon.
- Flaps: dorsal and volar random-pattern proximal flaps for webspace.
- Graft: FTSG from wrist crease for colour, no hair, less contracture. Incomplete syndactyly can often be closed with local flaps only.
- Nailfold: "stilleto flap" is a hyponychial interdigitating flap described by Buck-Gramcko or Hentz's "pulp plasty" with a composite graft.
- Sutures: use absorbable sutures.
- Defatting: reducse tension and graft requirements, and increases vascular injury.
The management plan is similar for complex syndactyly except that flaps not grafts should cover any bone or joints. In patients with syndromic syndactyly, for example, Aperts Syndrome, symphalangism can also be present. As a result, a zig-zag incision can be replaced with a straight-line incision.
Commisure Flap Design
There are a large number of flap designs for syndactyly reconstruction. This is one technique:
Dorsal:
- A "dorsal commisure flap".
- Aim: reconstruct the commisure.
- Design: metacarpal head to distal 2/3 proximal phalanx.
Volar:
- A "volar resurfacing rectangular flap".
- Aim: resurface proximal end of the digit that is adjacent to the commissure.
- Design: a proximal transverse incision that represents the level of commissure reconstruction, and the distal transverse edge equals the length of the dorsal commissure flap.
- This can also be performed as a "T-shaped" flap.
In the thumb-index webspace:
- Mild: four-flap Z-plasty (120 degrees) to access to adductor & first dorsal interosseous muscles (may require a partial release for adequate web-space breadth).
- Complete: modified dorsal rotation advancement flap by Abdel Ghani.
Contraindications for Syndactyly Release
Each patient should be managed as an individual. Generally speaking, relative contradindications include:
- Systemic comorbidities that make surgery unsafe.
- A severe complex or complicated syndactyly that could result in a poor functional status.
- Abnormal vasculatur that could compromise finger viability.
- Mild syndactyly that has no functional deficit.
- A hypoplastic digit that would become functionless if separated from a functional digit it is fused to.
Complications
Complications of syndactyly release can be intra-operative or post-operative and relate to the surgery or the anaesthetic.
- Peri-operative: nerve, tendon, artery, or vein injury; haematoma
- Wound: infection, dehiscence
- Scarring: hypertrophy, contracture, web creep (commissure pulled distally)
- Bone: joint instability due to insufficient collateral ligaments
- Nail: nail deformities
Venous complications are more common and often related to too tight a closure.
Conclusion
1. Basics of Syndactyly: You've gained a comprehensive understanding of syndactyly, a congenital hand malformation characterized by the fusion of two or more digits.
2. Classification Systems: You are now familiar with the classification of syndactyly, which distinguishes between simple and complex forms, as well as complete and incomplete types.
3. Diagnostic Approaches: You have learned that the diagnosis of syndactyly is primarily clinical, supported by radiological findings that confirm the presence of bone involvement and the extent of the fusion.
4. Management Strategies: You understand the management options for syndactyly, which range from surgical separation of fused digits to more complex reconstructive procedures depending on the severity of the condition.
5. Associated Conditions: You are aware that syndactyly can occur as an isolated condition or in association with various syndromes, and recognizing these associations is important for comprehensive patient care.
6. Surgical Techniques: You have an understanding of the specific surgical interventions used in the treatment of syndactyly, such as webspace creation, tendon and ligament reconstruction, and the use of skin grafts and flaps to achieve optimal functional and cosmetic outcomes.
