

Summary Card
Definition
A spectrum of unilateral congenital chest wall deformities involving the sternal head of the pectoralis major. It is associated with ipsilateral hand anomalies.
Aetiology
Poland syndrome occurs predominantly on the right side and mostly in males. The precise aetiology remains uncertain but working theories include subclavian artery hypoplasia, genetic and teratogenic.
Presentation
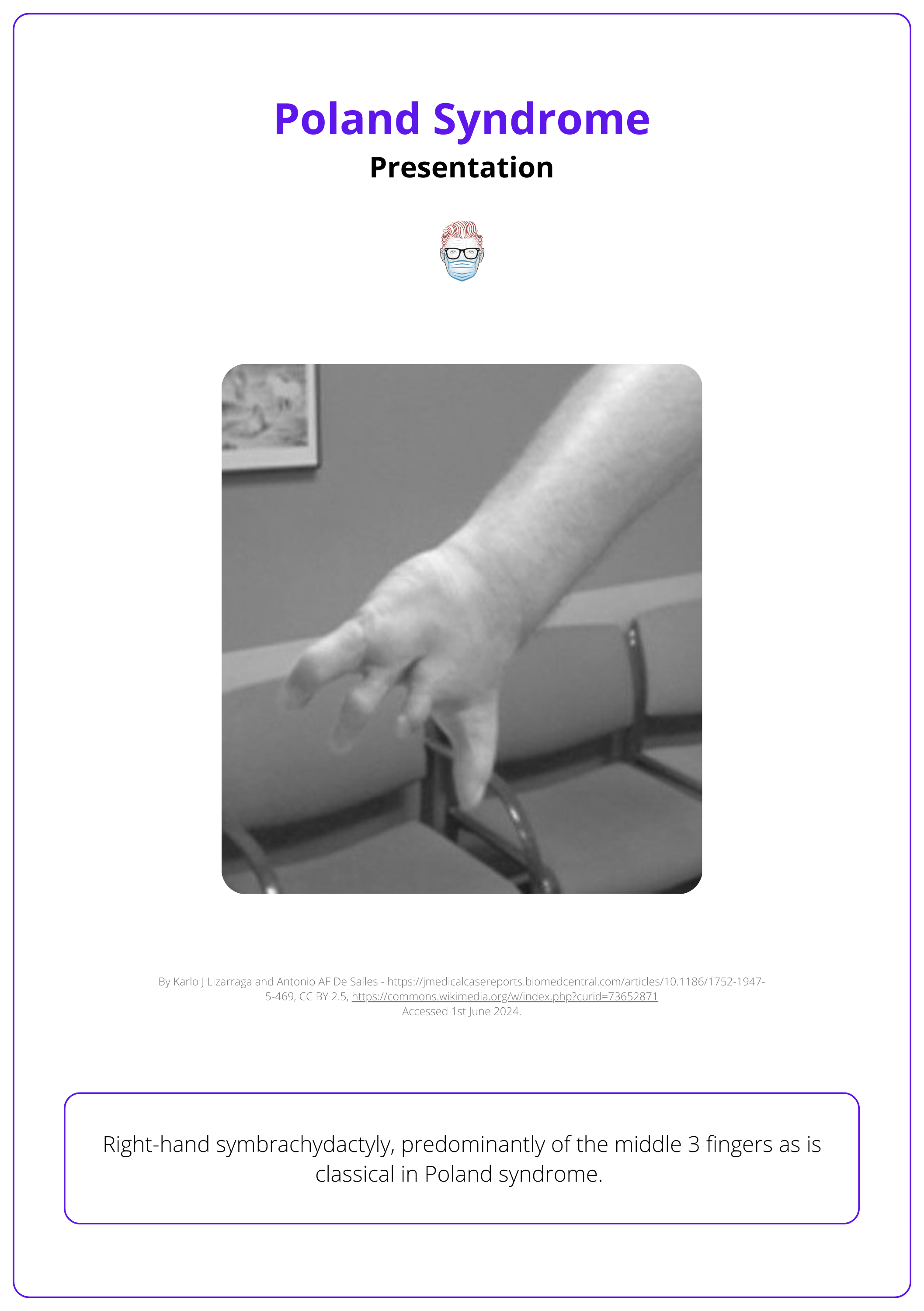
Poland syndrome is a constellation of phenotypes including the absence of hypoplasia of the sternal portion of the pectoralis major alongside predominantly ipsilateral chest wall and hand differences.
Investigations
Poland syndrome is a clinical diagnosis. Imaging is useful to exclude rare associations and for pre-operative planning.
Differential Diagnosis
The differential diagnosis of Poland syndrome depends on the structures involved - chest wall, shoulder, and hand. Rare syndromes and associations should be kept in mind.
Management
Surgical management aims to create a stable and symmetrical thorax and chest wall while optimising hand function and appearance.
Primary Contributor: Dr Suzanne Thomson, Educational Fellow.
Reviewer: Dr Kurt Lee Chircop, Educational Fellow.
Definition of Poland Syndrome
Poland syndrome is a unilateral congenital condition characterised by chest wall deformity, aplasia or hypoplasia of the pectoralis major and minor muscles, and ipsilateral hand anomalies among other features.
Poland syndrome refers to a spectrum of unilateral chest wall, shoulder and upper limb anomalies. It is usually sporadic, although a few familial cases have been described (Darian, 1989) and is more common in males.
Initial case reports were provided in 1826 (Moir, 2008), with the eponym being taken from Alfred Poland’s 1941 paper of an autopsy of a 27-year-old convict (Poland, 1941 & Ram 2015).
The image below further defines Poland syndrome.

75% of cases of Poland syndrome involve the right side.
Aetiology of Poland Syndrome
Poland syndrome occurs predominantly on the right side and mostly in males. The precise aetiology remains uncertain but working theories include subclavian artery hypoplasia, genetic and teratogenic.
Poland syndrome occurs in around 1:20,000 - 1:32,000 live births, with a male-to-female ratio of 3:1 (Gupta, 2000). The exact aetiology is unknown. It is generally considered to be:
- Sporadic (genetic associations have been described by Glass)
- “Subclavian-artery steal syndrome”: a unilateral reduction in blood supply due to a developmental difference in the subclavian artery.
- Drugs: Teratogens (Moir, 2008).Maternal smoking (doubles the risk), Cocaine, Misoprostol (prostaglandin analogue).
There have been a handful of cases described in the literature of Poland syndrome presenting in conjunction with Moebius syndrome (congenital hypoplasia of the 6th and 7th cranial nerves).
Genetic studies have identified PLXND1 as a possible causative gene linking the two congenital differences (Glass, 2022).
Presentation of Poland Syndrome
Poland syndrome is a constellation of phenotypes including the absence of hypoplasia of the sternal portion of the pectoralis major, alongside predominantly ipsilateral chest wall and hand differences.
Patients with Poland syndrome are most commonly referred for evaluation due to noticeable deformities in the hand or chest wall.
Clinical Features
The syndrome's most consistent feature across cases is the hypoplasia or aplasia of the sternal head of the pectoralis major.
- Chest wall: Aplasia or hypoplasia of the breast, hypoplastic scapula, rib hypoplasia
- Shoulder: Axillary bands, muscle hypoplasia
- Hand: Brachydactyly (short digits), Symbrachydactyly (short, joined or webbed digits), Syndactyly (joined or webbed digits), Ectrodactyly (absence of digits)
Associated Anomalies
While extremely rare, some cases of Poland syndrome have been associated with the development of childhood hematological and solid organ malignancies, including:
- Acute lymphoblastic leukemia
- Acute myeloblastic leukemia
- Chronic myelogenous leukemia
- Non-Hodgkin's lymphoma
There are also reports of Poland syndrome occurring alongside other congenital conditions such as:
- Craniofrontonasal dysplasia
- Pituitary anomalies
- Dextrocardia (Ozkok S, 2018).
Cardiorespiratory compromise secondary to deformity is uncommon.
The image below illustrates right-hand symbrachydactyly in the presentation of Poland syndrome.
Sprengel’s anomaly is the failure of the descent of the scapula. The scapula may also be hypoplastic and winged.
Investigations for Poland Syndrome
Poland syndrome is a clinical diagnosis. Imaging is useful to exclude rare associations and for pre-operative planning.
Poland syndrome is primarily diagnosed based on clinical observations. The role of diagnostic investigations is to confirm the extent of physical anomalies, exclude associated conditions, and assist in surgical planning.
Investigations to consider include:
- X-ray: Hands, chest wall, and shoulder girdle.
- US: Chest wall, shoulder, cardiac, abdominal, & renal (Baldelli I, 2020).
- CT or MRI: For 3D reconstruction and surgical planning.
- Genetic counselling and testing are not yet routine but may be offered.
Differential Diagnosis of Poland Syndrome
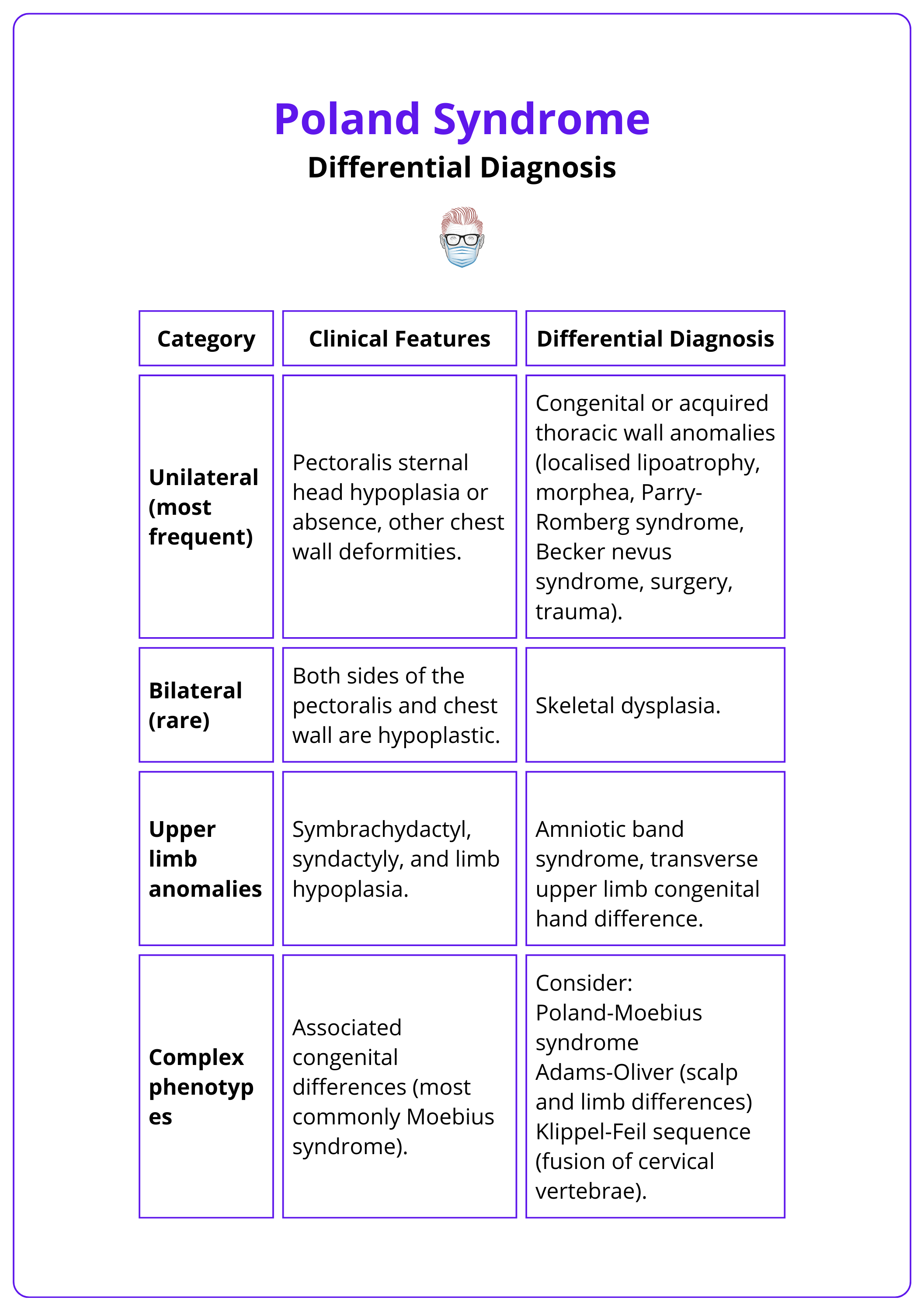
The diagnosis of Poland syndrome depends on the structures involved. Rare syndromes and associations should be kept in mind.
Poland syndrome may be considered in 4 categories:
- Unilateral
- Bilateral (rare)
- Associated upper limb anomalies
- Complex
These categories and their features are illustrated in the table below.
Management of Poland Syndrome
Surgical management aims to create a stable and symmetrical thorax and chest wall, whilst optimising hand function and appearance.
Management of Poland Syndrome involves a blend of surgical intervention and supportive therapies to address both the physical deformities and psychological impact of the condition:
- Non-progressive nature: Patients and families are reassured about the non-progressive nature of the diagnosis.
- Supportive therapies: Physiotherapy, occupational therapy, and psychological support are critical, particularly as children transition into young adulthood.
- Considerations for timing: Surgical interventions are planned around key developmental stages to minimize impact on self-esteem and body image, typically intensifying around age 6 or 7 and into the teenage years.
Surgical Interventions
Early surgical intervention is required in severe chest wall deformity that can be associated with lung herniation in around 7% of cases (Moir, 2008). Surgery may focus on the chest or upper limb and address functional and aesthetic concerns.
Individuals with isolated, mild chest wall differences may not desire any intervention but options should be discussed.
Reconstruction of Rib and Sternum Defects
A multidisciplinary approach with cardiothoracic surgeons is warranted for large defects. Key principles include delaying surgery until after growth spurts and addressing all tissue layers. The objectives are to ensure thoracic stability, protect pulmonary and mediastinal structures, prevent paradoxical chest wall motion, and support soft tissue reconstruction (breast or pectoralis).
- Goertex mesh +/- bone or cartilage graft
- Sternal osteotomy
- Nuss procedure for pectus excavatum
Reconstruction of the Shoulder Girdle, Anterior Axillary Fold, and Chest Wall
- Reconstruction of anterior axillary fold and pectoralis muscle: endoscopic/short incision pedicled latissimus dorsi – functional and aesthetic (Ouyang, 2021)
- Reconstruction of the breast: extended latissimus dorsi +/- fat grafting/implant or free tissue transfer (Pinsole, 2008).
Reconstruction of Hand Differences
Surgery is planned between 6 months and 3 years, depending on the digits involved. Ideal timing considers the child's size to avoid growth restriction from delayed operation (e.g., growth discrepancy in syndactyly), prioritization of associated anomalies requiring surgery, delays for safe general anesthesia, and avoiding conflicts with developmental milestones or significant life events.
- Symbrachydactyly: Surgical distraction or toe interphalangeal joint transfer (Lister, 1988, Schenker, 2003, Sabapathy 2021). Free toe transfer (Van Holder, 1999).
- Syndactyly: Surgical release of conjoined digits with or without skin graft (Choong, 2024).
When the ipsilateral latissimus dorsi muscle is unavailable for anterior chest wall reconstruction, the contralateral latissimus can be used as a functional free flap. Powered by the intercostal nerve, it restores pectoralis function, anterior chest wall symmetry, and posterior axillary fold symmetry. (Kelly, 1999).
Conclusion
1. Poland Syndrome: You have understood Poland Syndrome, recognizing it as a complex congenial condition characterized by a spectrum of anomalies primarily affecting the chest wall and upper limbs.
2. Clinical Features: You have identified the distinctive physical manifestations of Poland syndrome; hypoplasia or aplasia of the sternal head of the pectoralis major and minor muscles, and various hand anomalies.
3. Aetiology: You are familiar with theories concerning the origin of Poland Syndrome, suggesting a vascular disruption due to subclavian artery supply issues, alongside potential genetic and teratogenic influences.
4. Diagnostic Approach: You understand Poland Syndrome is primarily diagnosed through clinical evaluation, supported by imaging techniques in detailed assessment and pre-surgical planning.
5. Management Strategies: You have a clear outline of the management options, emphasizing surgical intervention aimed at correcting deformities to achieve functional and aesthetic improvements.
6. Differentiation from Similar Conditions: You can distinguish Poland Syndrome from other syndromes and anomalies based on the specific structures involved and its unique clinical presentations.
Further Reading
- Gupta A, Kay S, Sheker L. The Growing Hand: Diagnosis and Management of the Upper Extremity in Children: Diagnosis and Management of the Child's Upper Extremity - 2000 ISBN 10: 0723421331
- Kelly EJ, O'Sullivan ST, Kay SP. Microneurovascular transfer of contralateral latissimus dorsi in Poland's syndrome. Br J Plast Surg. 1999 Sep;52(6):503-4. doi: 10.1054/bjps.1999.3156. PMID: 10673931.
- Glass GE, Mohammedali S, Sivakumar B, Stotland MA, Abdulkader F, Prosser DO, Love DR. Poland-Möbius syndrome: a case report implicating a novel mutation of the PLXND1 gene and literature review. BMC Pediatr. 2022 Dec 30;22(1):745. doi: 10.1186/s12887-022-03803-3. PMID: 36581828; PMCID: PMC9801559.
- Darian VB, Argenta LC, Pasyk KA. Familial Poland's syndrome. Ann Plast Surg. 1989 Dec;23(6):531-7. doi: 10.1097/00000637-198912000-00010. PMID: 2560355.
- Ozkok S, Erol N, Onal C, Yikilmaz A. Left-sided Poland's syndrome associated with dextrocardia. North Clin Istanb. 2018 Sep 3;6(2):192-195. doi: 10.14744/nci.2018.82698. PMID: 31297489; PMCID: PMC6593920.
- Baldelli I, Baccarani A, Barone C, Bedeschi F, Bianca S, Calabrese O, Castori M, Catena N, Corain M, Costanzo S, Barbato GP, De Stefano S, Divizia MT, Feletti F, Formica M, Lando M, Lerone M, Lorenzetti F, Martinoli C, Mellini L, Nava MB, Porcellini G, Puliti A, Romanini MV, Rondoni F, Santi P, Sartini S, Senes F, Spada L, Tarani L, Valle M, Venturino C, Zaottini F, Torre M, Crimi M. Consensus-based recommendations for diagnosis and medical management of Poland syndrome (sequence). Orphanet J Rare Dis. 2020 Aug 5;15(1):201. doi: 10.1186/s13023-020-01481-x. PMID: 32758259; PMCID: PMC7405453.
- Nguyen GV, Goncalves LF, Vaughn J, Friedman N, Wickland J, Cornejo P. Prenatal diagnosis of Poland-Möbius syndrome by multimodality fetal imaging. Pediatr Radiol. 2023 Sep;53(10):2144-2148. doi: 10.1007/s00247-023-05712-8. Epub 2023 Jul 10. PMID: 37423914.
- Moir CR, Johnson CH. Poland's syndrome. Semin Pediatr Surg. 2008 Aug;17(3):161-6. doi: 10.1053/j.sempedsurg.2008.03.005. PMID: 18582821.
- Poland A. Deficiency of the pectoral muscles. Guy’s Hosp Rep 1841; 6:191 in Ram AN, Chung KC. Poland's syndrome: current thoughts in the setting of a controversy. Plast Reconstr Surg. 2009 Mar;123(3):949-953. doi: 10.1097/PRS.0b013e318199f508. PMID: 19319059; PMCID: PMC4410274.
- Ouyang Y, Xu B, Luan J, Liu C. Chest Wall Reconstruction in Male Poland Syndrome Patients with Endoscopic-Assisted Latissimus Dorsi Muscle Flap Transfer. J Plast Reconstr Aesthet Surg. 2021 Nov;74(11):3141-3149. doi: 10.1016/j.bjps.2021.03.117. Epub 2021 May 4. PMID: 34039526.
- Pinsolle V, Chichery A, Grolleau JL, Chavoin JP. Autologous fat injection in Poland's syndrome. J Plast Reconstr Aesthet Surg. 2008 Jul;61(7):784-91. doi: 10.1016/j.bjps.2007.11.033. Epub 2008 Feb 21. PMID: 18178141.
- Lister G. Microsurgical transfer of the second toe for congenital deficiency of the thumb. Plast Reconstr Surg. 1988 Oct;82(4):658-65. doi: 10.1097/00006534-198810000-00017. PMID: 3420188.
- Choong J, Hadjiandreou M, McGee P, Lam WL. Graftless Syndactyly Release. Tech Hand Up Extrem Surg. 2024 Jun 1;28(2):51-59. doi: 10.1097/BTH.0000000000000472. PMID: 38764415.
- Sabapathy SR, Mohan M, Shanmugakrishnan RR. Nonvascularized Free Toe Phalangeal Transfers in Congenital Hand Differences: Radiological, Functional, and Patient/Parent-Reported Outcomes. J Hand Surg Am. 2021 Dec;46(12):1124.e1-1124.e9. doi: 10.1016/j.jhsa.2021.03.012. Epub 2021 May 7. PMID: 33966936.
- Schenker M, Kelley SP, Kay SP. Free hand-to-toe transfer: a method to minimise donor-site morbidity in free joint transfers. Br J Plast Surg. 2003 Jan;56(1):57-9. doi: 10.1016/s0007-1226(03)00003-1. PMID: 12706156.
- Van Holder C, Giele H, Gilbert A. Double second toe transfer in congenital hand anomalies. J Hand Surg Br. 1999 Aug;24(4):471-5. doi: 10.1054/jhsb.1999.0162. PMID: 10473161.
- Chavoin JP, Taizou M, Moreno B, Leyx P, Grolleau JL, Chaput B. Correcting Poland Syndrome with a Custom-Made Silicone Implant: Contribution of Three-Dimensional Computer-Aided Design Reconstruction. Plast Reconstr Surg. 2018 Aug;142(2):109e-119e. doi: 10.1097/PRS.0000000000004605. PMID: 30045173.
