

Summary Card
Overview
In median nerve pathology, tendon transfer restores thumb opposition and flexion of the thumb, index, and middle fingers.
Anatomy
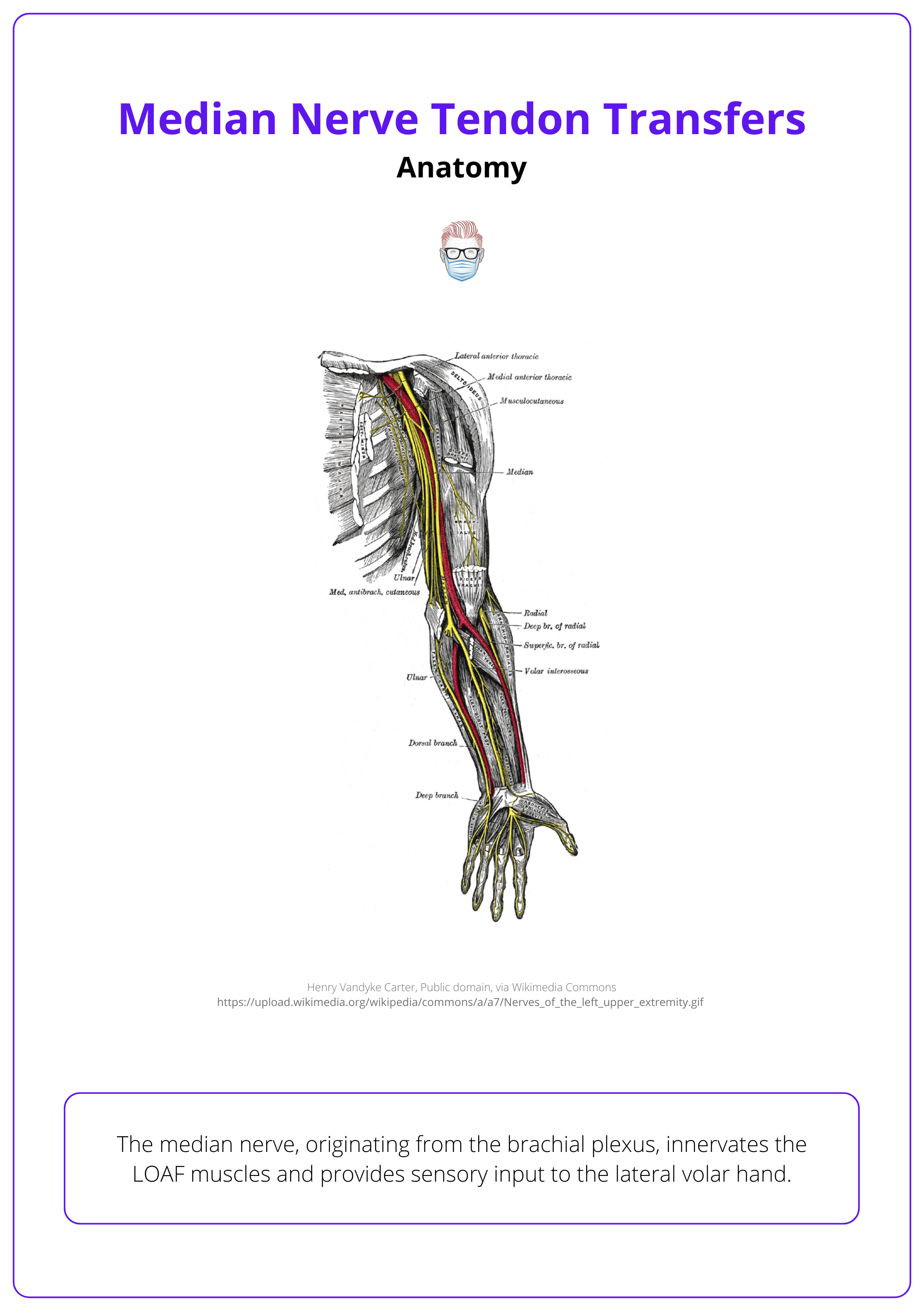
The median nerve, originating from the brachial plexus, innervates the LOAF muscles and provides sensory input to the lateral volar hand.
Principles
There are key principles of tendon transfer surgery that guide optimal outcomes. Consider the function that has been lost, the available donor tendons, and the priorities for restoration.
Indications
High median nerve palsy impacts pronation, wrist, lateral digit flexion, and opposition, whereas low median nerve palsy impacts only opposition.
Management
If conservative treatment has been exhausted, tendon transfers from radial and ulnar nerve-innervated muscles can restore opposition, pinch, and finger flexion.
Primary Contributor: Dr Suzanne Thomson, Educational Fellow.
Reviewer: Dr Kurt Lee Chircop, Educational Fellow.
Overview of Median Nerve Tendon Transfers
Tendon transfer relocates a muscle-tendon unit to restore lost movement. In median nerve pathology, it restores thumb opposition and flexion of the index, middle fingers, and thumb.
A tendon transfer involves moving a muscle-tendon unit to a new location to restore or improve movement and function. This technique redirects a working tendon to optimize its mechanical advantage, enhancing functional outcomes.
Initially developed for obstetric brachial plexus palsies and polio, tendon transfers became more prominent in:
- World War I with Jones, Meyer, and Steindler
- World War II with Boyes, Bunnell, and Zancolli
- 1949 with Littler, who popularized the method (Littler, 1949).
The image below illustrates the median nerve and median nerve innervated muscles.
Galen advised against suturing tendons due to their link to nerves, a view that prevailed until tendon transfer surgery emerged in the 1800s.
Anatomy of the Median Nerve
The median nerve, originating from the brachial plexus, innervates the LOAF muscles and provides sensory input to the lateral volar hand.
Overview
The median nerve originates from the lateral (C5-7) and medial (C8-T1) cords of the brachial plexus. It runs alongside the brachial artery, passes under the bicipital aponeurosis, and travels between the two heads of the pronator teres.
It continues deep to the flexor digitorum superficialis (FDS), where the anterior interosseous nerve (AIN) branches off to the following muscles:
- Flexor pollicis longus (FPL)
- Flexor digitorum profundus (FDP) to the index and middle fingers
- Pronator quadratus (PQ)
Before entering the carpal tunnel, the median nerve gives off the palmar sensory branch for the palm. Inside the carpal tunnel, it divides into:
- Recurrent Motor Branch: LOAF muscles—1st and 2nd lumbricals, opponens pollicis, abductor pollicis brevis, and flexor pollicis brevis. This branch varies in its pattern.
- Sensory Branch: radial volar half of the hand.
Anatomy of the median nerve is illustrated below.
Branches of the Median Nerve (Proximal to Distal)
The median nerve branches proximally to distally, supplying forearm and hand muscles, including the anterior interosseous and recurrent motor branches.
"Proper" Median Nerve
- Articular branch to elbow
- Palmaris longus
- Pronator teres
- Flexor carpi radialis (FCR)
- All of FDS
Recurrent motor branch
- Lumbricals (1st and 2nd)
- Opponens pollicis
- Abductor pollicis brevis
- Flexor pollicis brevis (ulnar nerve innervates deep head)
Anterior interosseous branch:
- FPL
- FDP to index and middle fingers
- PQ
Principles of Median Nerve Tendon Transfers
There are key principles of tendon transfer surgery that guide optimal outcomes. Consider the function that has been lost, the available donor tendons, and the priorities for restoration.
Successful tendon transfers should be considered before muscle atrophy occurs in acute denervation for median nerve injuries, hingeing on a few key principles.
- Understanding the lost function.
- Identifying suitable donor tendons.
- Prioritising functional restoration.
General Principles
- Soft Tissue and Joint Preparation
- Ensure good soft tissue coverage.
- Achieve full joint range of motion before tendon transfer.
- Stabilize non-functional joints through muscles or arthrodesis.
- Donor Tendon Selection
- Use expendable tendons that don’t compromise essential functions.
- Match donor muscle power and amplitude to the lost function (e.g., using pronator teres for extensor carpi radialis brevis).
- Select muscles with sufficient excursion: approximately 3 cm for ECU/FCU/FCR, 5 cm for EDC/FPL/EPL, and 7 cm for FDS/FDP.
- Prefer synergistic muscle pairs (e.g., wrist flexors for finger extensors).
- Specific Considerations for Median Nerve Injuries
- Low Median Nerve Injury: Focus on reconstructing thumb opposition.
- High Median Nerve Injury: Requires reconstruction of thumb opposition and flexion of the index and middle fingers.
Nerve transfers can also restore sensation, aiding in functional hand use (e.g., brachioradialis to the anterior interosseous nerve) (MacKinnon, 2019).
The Blix curve describes muscle power relative to length. A muscle can shorten 40% before output ceases and stretch 40% before rupture (Gardenier, 2020).
Indications for Median Nerve Tendon Transfer
A tendon transfer may be indicated secondary to neurological or musculoskeletal pathology or trauma.
Tendon transfers for median nerve injuries are typically indicated due to neurological, musculoskeletal, or traumatic causes, aiming to restore lost functions such as thumb opposition, finger flexion, and forearm pronation.
Common Causes of Median Nerve Injuries
- Neurological Conditions
- Compressive neuropathies (e.g., carpal tunnel syndrome, lacertus fibrosis)
- Penetrating trauma (e.g., lacerations)
- Conditions like polio, cerebrovascular accidents (CVA), tetraplegia
- Congenital issues such as brachial plexus palsy
- Muscle and Tendon Pathology
- Trauma leading to muscle or tendon damage
- Ischemic events causing necrosis
- Tumors affecting nerve or tendon structures
- Chronic conditions, like rheumatoid arthritis, cause tendon rupture
Double crush syndrome involves nerve compression at multiple sites. Hagerty et al. found lacertus fibrosus compression in 78% of carpal tunnel cases during median nerve decompression (Kong, 2023).
High vs Low
Clinical assessment should distinguish between high and low median nerve palsy.
- High Median Nerve Palsy: Loss of forearm pronation, wrist radial deviation, thumb IPJ flexion, PIPJ flexion in all fingers, DIPJ flexion in the index and middle fingers, and thumb opposition.
- Low Median Nerve Palsy: Loss of thumb opposition only.
In chronic carpal tunnel syndrome, severe atrophy of the APB muscle may require tendon transfer to restore thumb opposition.
Management of Median Nerve Tendon Transfers
If conservative treatment fails, tendon transfers from radial and ulnar nerve-innervated muscles can restore opposition, pinch, and finger flexion.
Initial supportive management includes splinting, physiotherapy, and occupational therapy. If there is no chance of nerve recovery, a tendon transfer is indicated.
Opponensplasty
Various techniques transfer a donor tendon to the abductor pollicis brevis (APB) insertion, with the choice depending on donor muscle function and patient needs:
- Palmaris longus (Camitz procedure): Routed through the transverse carpal ligament to create a pulley.
- Abductor digiti minimi (Huber): Common in pediatric cases, may cause loss of the palmar valley.
- Flexor digitorum superficialis to ring finger (Thompson-Royle).
- Extensor indicis proprius (Burkhalter's popularised technique).
EIP Opponesplasty
Thumb IPJ Flexion
- Brachioradialis to flexor pollicis longus (FPL).
Index and Middle Finger Flexion
- Side-to-side transfer of little and ring finger flexor digitorum profundus (FDP) to the index and middle fingers.
Altering the location and design of pulleys in tendon transfers can change the pull direction and friction levels, enhancing tendon gliding (Duymaz, 2013).
Post-Operative Care
Optimal follow up care to protect the repair whilst optimising range and glide of movement should be guided by a close working relationship between patient, surgeon, OT and PT.
Initial splinting protects the repair followed by tendon gliding and relearning exercises provided (Ratner JA, 2010).
Conclusion
1. Overview of Tendon Transfers: Discussed the historical evolution and technical application of tendon transfers.
2. Median Nerve Anatomy and Function: Explained the anatomical pathway, key muscular innervations, and the median nerve's critical role in hand and finger movements.
3. Principles for Tendon Transfers: Outlined essential considerations for effective tendon transfer surgeries.
4. Causes of Median Nerve Injuries: Identified potential neurological, musculoskeletal, or traumatic causes leading to median nerve injuries.
5. Symptoms and Diagnostic Approach: Reviewed how median nerve palsy presents and the specific tests used to diagnose the extent of nerve damage.
6. Tendon Transfer Procedures: Detailed surgical techniques to restore crucial hand functions, depending on the severity and location of the nerve injury.
7. Post-Operative Care and Outcomes: Emphasized the importance of coordinated post-operative care.
Further Reading
- LITTLER JW. Tendon transfers and arthrodeses in combined median and ulnar nerve paralysis. J Bone Joint Surg Am. 1949 Apr;31A(2):225-34. PMID: 18116560.
- https://youtu.be/r3Hxtl9wJjk?feature=shared
- Gardenier J, Garg R, Mudgal C. Upper Extremity Tendon Transfers: A Brief Review of History, Common Applications, and Technical Tips. Indian J Plast Surg. 2020 Aug;53(2):177-190. doi: 10.1055/s-0040-1716456. Epub 2020 Aug 29. PMID: 32884184; PMCID: PMC7458847.
- Ducic I, Dellon AL, Bogue DP. Radial sensory neurotization of the thumb and index finger for prehension after proximal median and ulnar nerve injuries. J Reconstr Microsurg. 2006 Feb;22(2):73-8. doi: 10.1055/s-2006-932500. PMID: 16456766.
- Kong G, Brutus JP, Vo TT, Hagert E. The prevalence of double- and multiple crush syndromes in patients surgically treated for peripheral nerve compression in the upper limb. Hand Surg Rehabil. 2023 Dec;42(6):475-481. doi: 10.1016/j.hansur.2023.09.002. Epub 2023 Sep 14. PMID: 37714514.
- Sammer DM, Chung KC. Tendon transfers: Part II. Transfers for ulnar nerve palsy and median nerve palsy. Plast Reconstr Surg. 2009 Sep;124(3):212e-221e. doi: 10.1097/PRS.0b013e3181b037c7. PMID: 19730287; PMCID: PMC2741332.
- Ratner JA, Peljovich A, Kozin SH. Update on tendon transfers for peripheral nerve injuries. J Hand Surg Am. 2010 Aug;35(8):1371-81. doi: 10.1016/j.jhsa.2010.05.023. PMID: 20684937.
- Duymaz A, Karabekmez FE, Zhao C, An KN, Amadio PC, Moran SL. Tendon transfer for the restoration of thumb opposition: the effects of friction and pulley location. Plast Reconstr Surg. 2013 Sep;132(3):604-609. doi: 10.1097/PRS.0b013e31829ad20e. PMID: 23985635.
- Brand PW. Tendon transfers for median and ulnar nerve paralysis. Orthop Clin North Am. 1970 Nov;1(2):447-54. PMID: 5521866.
