

Summary Card
Definition of Thumb Hypoplasia
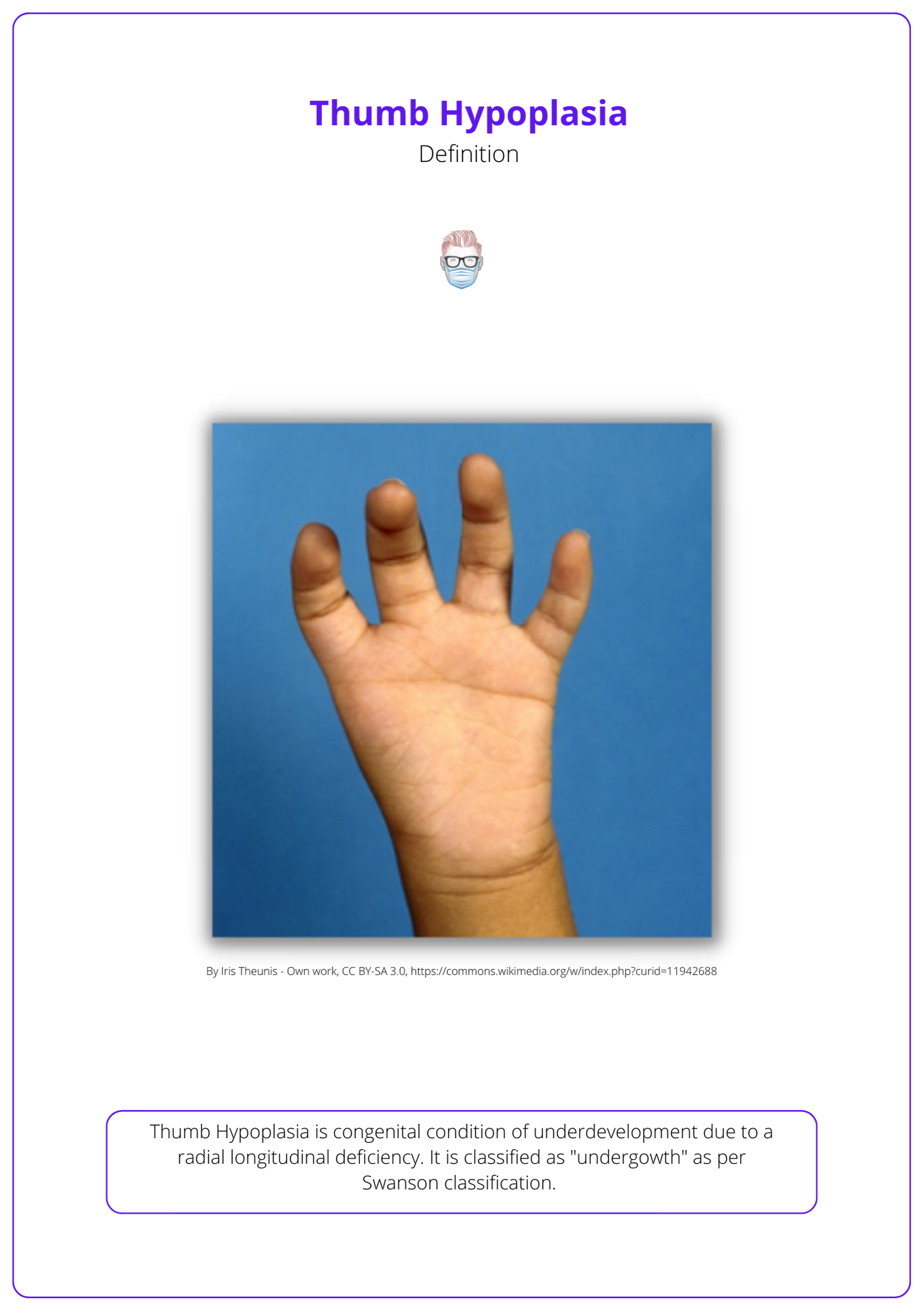
Congenital thumb "undergrowth" due to a radial longitudinal deficiency.
Diagnosis of Thumb Hypoplasia
A clinical diagnosis supported by radiology and specific investigations for associated anomalies.
Classification of Thumb Hypoplasia
Blath Classification from I (functional small thumb) to V (absent thumb). This guides management.
Staged Reconstruction of Thumb Hypoplasia
Indicated in Blauth II and IUIa for webspace release, UCL reconstruction, opponensplasty, and tendon reconstruction.
Index Pollicisation for Thumb Hypoplasia
Indicated for Blauth IIIb, IV, or V.
Definition of Thumb Hypoplasia
Thumb Hypoplasia is the congenital underdevelopment of the thumb due to a radial longitudinal deficiency. It is classified as "undergrowth" as per the Swanson classification. This is illustrated below.
Diagnosis of Thumb Hypoplasia
Thumb hypoplasia is a clinical diagnosis supported by radiological investigations. Further investigations may be required for associated conditions.
Clinical Diagnosis
Thumb hypoplasia is a clinical diagnosis based on findings during clinical inspection and assessment of the range of motion. It can be supported by radiological findings.
- Skin: Absent skin creases, web-space tightness.
- Ligaments: Excessive abduction of MCP joint in UCL insufficiency.
- Muscles: Hypoplasia of thenar musculature.
- Tendons: Pollex abductus (FPL has extra insertion onto extensor tendon).
- Movement: UCL laxity, absence of motion at joints (Blauth III).
These clinical features of thumb hypoplasia are illustrated below.

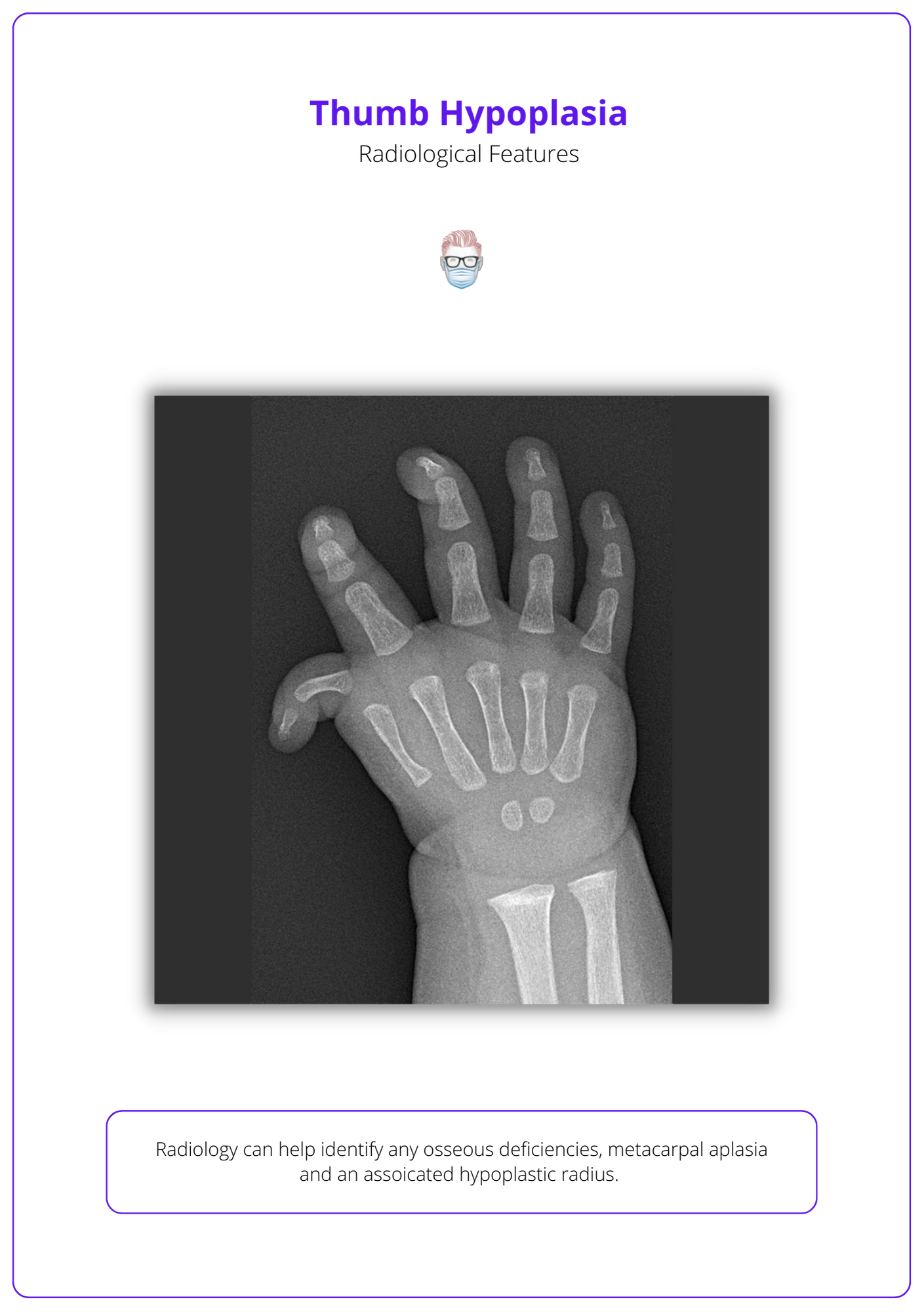
Radiological Findings
It is recommended to request bilateral films of the hand, wrist, and forearm.
- Can help determine musculotendinous versus osseous deficiencies.
- Type III B Basal metacarpal aplasia with deficient CMC joint.
- Any associated hypoplastic radius.
Associated Conditions
Thumb hypoplasia can be associated with a diverse group of genetic conditions and syndromes. These include:
- VACTERL: Vertebral anomalies, Anal atresia, Cardiac defects, Tracheal anomalies, Esophageal atresia, Renal and radial abnormalities, Limb abnormalities.
- Holt-Oram: Autosomal dominant, upper-limb defects, congenital heart malformation, cardiac conduction disease. Common cardiac defects include atrial or ventricular septal defects and conduction abnormalities or blocks.
- Thrombocytopenia-absent radius: Bilateral absence of the radii with the presence of both thumbs and thrombocytopenia. It can be distinguished from Fanconi anemia by the neonatal onset of thrombocytopenia, which is typically seen later in life with Fanconi anemia, and the absence of pancytopenia.
- Fanconi anaemia: Autosomal recessive condiciton characterized by bone marrow failure and radial limb abnormalities. Other common anomalies include café au lait spots, short stature, genital abnormalities, and microcephaly. Patients usually die of complications from pancytopenia, with a life expectancy of 20-30 years. It can be diagnosed on peripheral blood smear, complete blood count, and chromosomal challenge test.
Classification of Thumb Hypoplasia
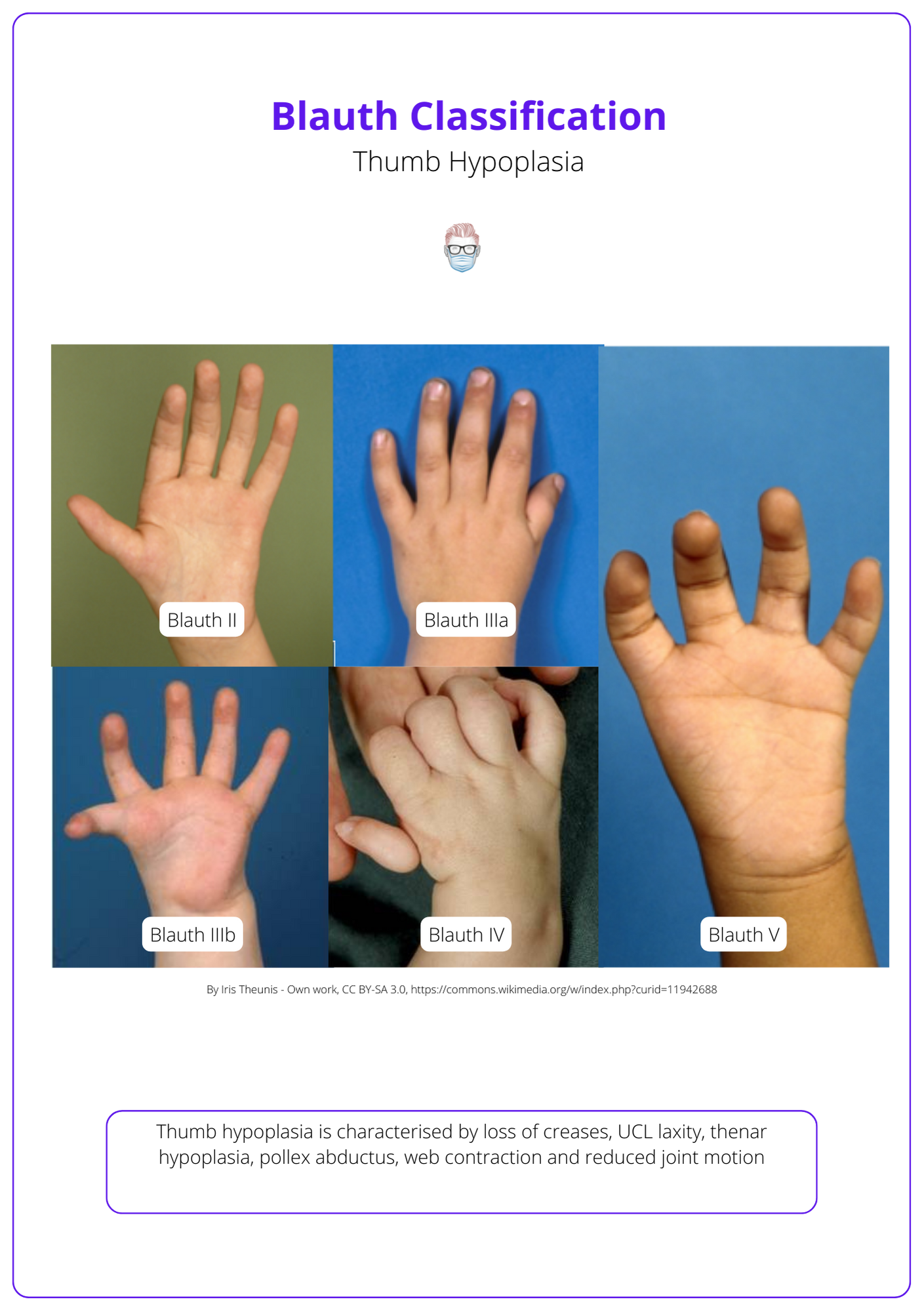
The Blauth classification is used in thumb hypoplasia to describe the severity of the condition and structures involved. It can be used as a template to guide management.
The Blauth Classification is used in thumb hypoplasia. It stratifies patients based on the degree of hypoplasia, collateral ligament, muscle, and tendon pathology.
- Blauth I: Functional hypoplastic thumb, normal neurovascular bundles,
- Blauth II: UCL insufficiency, webspace contracted, thenar hypoplasia.
- Blauth IIIa: Type II + abnormal extrinsic tendons + stable CMCJ.
- Blauth IIIb: Type II + abnormal extrinsic tendons + unstable CMCJ.
- Blauth IV: Floating thumb (pouce flottant) attached by a soft tissue bridge.
- Blauth V: Absent thumb.
This classification subsequently guides the reconstructive pathway for conservative, staged procedures or index pollicisation. Here are some general principles.
- Blauth I: if good function then does not require surgery
- Blauth II + IIIA: staged procedure for each abnormality
- Blauth IIIb: Pollicisation
Staged Reconstruction of Thumb Hypoplasia
Staged reconstruction is indicated in patients with a stable MCPJ (Blauth II, IIIa). It involves first web space release, UCL reconstruction, opponensplasty, and tendon reconstruction.
Thumb hypoplasia is usually surgically corrected by age 2 when indicated. A staged correction is indicated for Type II and IIIB thumb hypoplasia. This involves reconstruction of the webspace, MCPJ UCL insufficiency, hypothenar hypoplasia, and extrinsic tendons.
First Webspace Release
- This can be performed through a Z-plasty (e.g. a four-flap Z-plasty).
UCL Reconstruction
UCL deficiency may be primary or secondary to a pollex abductus (FPL inserts into the distal phalanx and the EPL). This can be treated by,
- Fusion
- UCL reconstruction with a tendon graft (if UCL remnant present)
- UCL reconstruction with FDS opponensplasty
Opponensplasty
This stage aims to augment the hypoplastic hypothenar muscles. Options for this opponensplasty include,
- Ring Finger FDS transfer (can also help reconstruct the UCL)
- Huber transfer (ADM to APB)
Tendon Reconstruction
Type III thumb hypoplasia has abnormal extrinsic tendons with a stable MCPJ. These patients can receive,
- EIP to EPL tendon transfer
- Pulley reconstruction
Index Pollicisation for Thumb Hypoplasia
Index pollicisation is indicated in Blauth IIIb, IV, and V thumb hypoplasia.
Index pollicisation is indicated in Blauth IIIB, IV, and V thumb hypoplasia. The fundamental goal is to recreate a functional thumb by utilizing a shortened and rotated index finger.
Incisions
- Radial palmer incision to create skin flaps at the base of the index finger that can be used to create a first webspace.
- Dorsal incisions should preserve dorsal draining veins.
Dissection
- Ulnar digital nerve is mobilisation by interfasciular dissection of the common digital nerve to the index-middle finger web.
- The radial digital artery to the middle finger is ligated and divided.
- Interossei are elevated from the index finger metacarpal.
Resections
- Index metacarpal is removed with its head preserved to form a trapezium.
- Epiphysis excised to prevent subsequent growth.
Stability
- The metacarpal head is rotated and secured with K-wires.
- 120-160° rotation, 40° palmar abduction with the MCPJ hyperextended.
Intrinsic and Extrinsic Rebalance
- Extrinsic shortened: FPL and EPL are trimmed to the length of the metacarpal.
- First dorsal interosseous to radial lateral band = APB.
- First palmar interosseous to ulnar lateral band = Adductor pollicis.
- EIP acts as EPL.
- EDC to index acts as APL.
Conclusion
1. Understanding of Thumb Hypoplasia: You have understood thumb hypoplasia, a congenital condition characterized by the underdevelopment of the thumb due to radial longitudinal deficiency.
2. Diagnostic Techniques: You now know how thumb hypoplasia is diagnosed, combining clinical examination with radiological investigations to assess the extent of the underdevelopment and any associated anomalies.
3. Classification Systems: You are familiar with the Blauth Classification. This classification aids in guiding the management strategies for each specific type.
4. Management Options: You have learned about management strategies for thumb hypoplasia. These treatments are tailored based on the severity of the hypoplasia as defined by the Blauth Classification.
5. Associated Conditions: You are aware that thumb hypoplasia can be associated with several genetic conditions and syndromes, prompting the need for a comprehensive evaluation of associated anomalies.
6. Surgical Techniques: You have been introduced to specific surgical interventions such as webspace release, UCL reconstruction, opponensplasty, and tendon reconstruction, as well as the complex procedure of index pollicisation.
