
In this Article
5 Key Points
- Gustilo Anderson Classification is most common grading system for open (or compound) fractures.
- Gustilo Anderson Classification was was first described in 1976 and later modified in 1987.
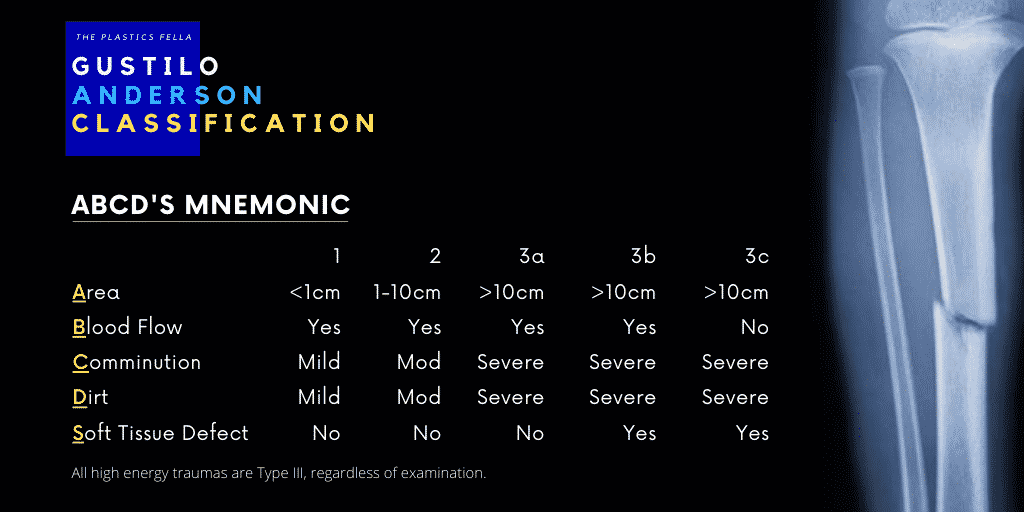
- The ABCD’s mnemonic is an easy way to remember the Gustilo Anderson Classification: area, blood, communition, dirt, soft-tissue.
- Ideally, open fractures should be used after debridement and in conjunction with other scoring systems, for example MESS.
- Scoring systems help guide open fracture definitive management, antibiotics , bone fixation and flap reconstructive options.
Gustilo-Anderson Classification
The Gustilo-Anderson Classification was first described in 19761 and later modified in 19872. The purpose is to provide a prognostic and communicative framework that guides best management options.
Mnemonic
The Gustilo-Anderson Classification mnemonic is be simplified in following table:
| Grade | Area | Blood | Comminuted | Dirt | Soft Tissue | Abx |
|---|---|---|---|---|---|---|
| 1 | ≤ 1 cm | Yes | – Minimal – No Stripping | Mild | – Minimal – Close | 1st gen. cephalosporin |
| 2 | 1-10cm | Yes | – Moderate – Minor Stripping | Mod. | – Minor – Close | 1st gen. cephalosporin |
| 3a | >10 cm | Yes | – Severe – Stripping | Severe | – Mod – Close | 1st gen. cephalosporin Aminoglycoside Penicillin |
| 3b | >10 cm | Yes | – Severe – Stripping | Severe | – Severe – Flap | 1st gen. cephalosporin Aminoglycoside Penicillin |
| 3c | >10 cm | – No – Revasc | – Severe – Stripping | Severe | – Severe – Flap | 1st gen. cephalosporin Aminoglycoside Penicillin |
All high energy traumas are Type III, regardless of the examination. This should be used to guide the soft tissue reconstruction algorithm as per BAPRAS Guidelines.
Memory Hook
In addition to the above mnemonic, a simple practical way to remember the Gustilo Anderson Classification is:
- 1cm or less wound that is clean
- 2cm or more wound that is relatively clean
- Segmental fracture, or open fracture with extensive soft tissue injury
- A: Adequate soft tissue
- B: Bad soft-tissue
- C: Circulation issues
Injuries classified as Gustilo-Anderson 3B, are now sub-classified into 1,2,3 based on the number of patent vessels, respectively.
Seminal Papers
The original 1976 publication1 included a retrospective study of 673 open fractures of long bones in 602 patients to determine the impact of primary versus secondary closure, use of primary internal fixation, and routine use of antibiotics in the treatment algorithm of open long-bone fractures.
The key findings were:
- Primary closure without primary internal fixation and prophylactic antibiotics for Type I and Type II open fractures reduced the risk of infection as much as 84.4%
- Acute internal fixation and primary closure after segmental fractures, extensive lacerations, avulsion, or traumatic amputation resulted in a greater likelihood of subsequent osteomyelitis.
This was then prospectively reviewed in the 1984 publication2 in 350 patients.
Discussion Points
The Gustilo-Anderson Classification, in spite of its widespread use, has been thoroughly examined in terms of validity, reproducibility and limitations. Here is a summary of those key points:
| Positive | Negative |
|---|---|
| Prognostic Indicator3–5 | Inter-observer variability6,7 |
| Widespread use allowing easier communication | The surface injury does not reflect deeper tissue damage8 |
| Standardised research tool | Limitations in original studies design |
Limitations and Controversy of Gustilo-Anderson Classification for Lower Limb Fractures
References
- 1. Gustilo R, Anderson J. Prevention of infection in the treatment of one thousand and twenty-five open fractures of long bones: retrospective and prospective analyses. J Bone Joint Surg Am. 1976;58(4):453-458. https://www.ncbi.nlm.nih.gov/pubmed/773941
- 2. GUSTILO RB, MENDOZA RM, WILLIAMS DN. Problems in the Management of Type III (Severe) Open Fractures. The Journal of Trauma: Injury, Infection, and Critical Care. Published online August 1984:742-746. doi:10.1097/00005373-198408000-00009
- 3. Caudle R, Stern P. Severe open fractures of the tibia. J Bone Joint Surg Am. 1987;69(6):801-807. https://www.ncbi.nlm.nih.gov/pubmed/3597491
- 4. Court-Brown C, Rimmer S, Prakash U, McQueen M. The epidemiology of open long bone fractures. Injury. 1998;29(7):529-534. doi:10.1016/s0020-1383(98)00125-9
- 5. Hansen S. The type-IIIC tibial fracture. Salvage or amputation. J Bone Joint Surg Am. 1987;69(6):799-800. https://www.ncbi.nlm.nih.gov/pubmed/3597490
- 6. Brumback R, Jones A. Interobserver agreement in the classification of open fractures of the tibia. The results of a survey of two hundred and forty-five orthopaedic surgeons. J Bone Joint Surg Am. 1994;76(8):1162-1166. doi:10.2106/00004623-199408000-00006
- 7. Horn B, Rettig M. Interobserver reliability in the Gustilo and Anderson classification of open fractures. J Orthop Trauma. 1993;7(4):357-360. doi:10.1097/00005131-199308000-00012
- 8. Kim PH, Leopold SS. Gustilo-Anderson Classification. Clin Orthop Relat Res. Published online May 9, 2012:3270-3274. doi:10.1007/s11999-012-2376-6