

👇 On this page
Inhalation injuries are defined as an airway's thermal or chemical exposure to a burn, the systemic effects and its complications.
It should be suspected in burns in an enclosed environment, diagnosed on examination, and supported by investigations.
They can be classified as supraglottic (usually direct thermal burn) or subglottic (usually a chemical exposure)
Treatment focuses on optimising the airway, fluid resuscitation, medical stabilisation, and burn management.
Carbon Monoxide poisoning is a by-product of incomplete combustion and is treated with high-flow oxygen.
Flashcards
Evidence-based, verified flashcards to improve your active recall.
Pathophysiology of Inhalation Injuries
Key Point
Inhalation injury refers to an airway's thermal or chemical exposure to a burn, the systemic effects and related complications.
Inhalation injury refers to the injury to an airway from a thermal burn or chemical exposure, the systemic effects and complications. More specifically:
- Direct local thermal and chemical exposures
- Systemic effects of inhaled toxins and burns
- Inflammatory and immune responses
- Secondary complications and clinical sequelae
The local pulmonary effects of the inflammatory responses include bronchospasm and vasospasm, bronchorrhea and alveolar flooding, bronchial exudate and cast formation, and ventilation-perfusion mismatching.
Inhalation Injury Diagnosis
Key Point
Inhalation injury should be considered in all patients with a history of fire in an enclosed space or unconscious. It is a clinical diagnosis supported by baseline investigations.
Clinical Picture
Assessing the clinical presentation is the most reliable method of diagnosis and approximate grading of severity (Ryan et al, 2012). Inhalation injury should be considered in all patients with a history of fire in an enclosed space or unconscious.
Patients with inhalation injuries may have the following symptoms:
- Speaking: hoarse or weak
- Coughing: heavy and brassy
- Breathing: Difficult, shortness of breath
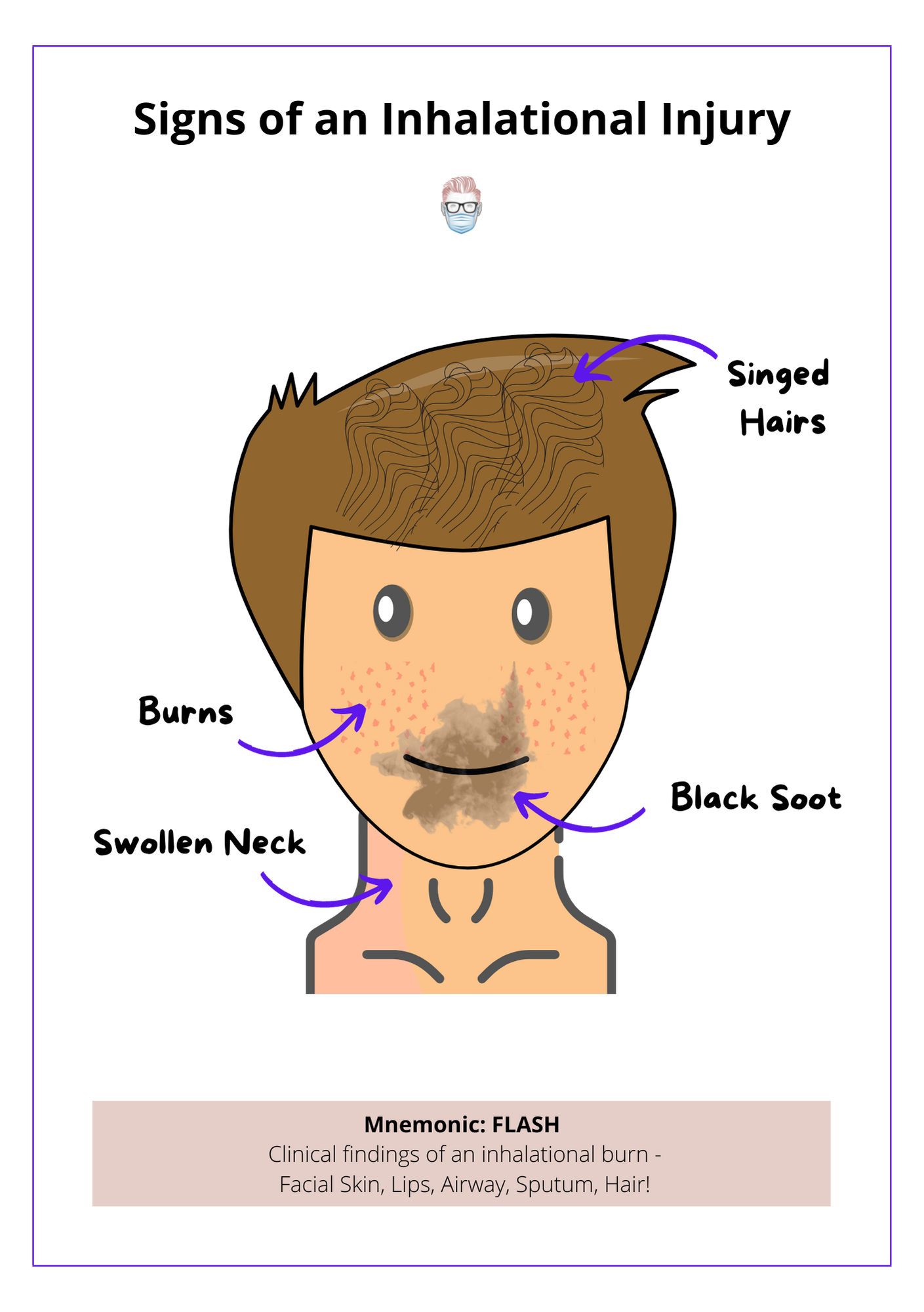
On examination, the following clinical findings may be present:
- Facial skin: burns
- Lips/Mouth: soot
- Airway: stridor, swelling.
- Sputum: carbonaceous/black
- Hair: singed
Investigations
Baseline and specialized investigations can help confirm an inhalational injury.
- Vital Signs: increase respiratory rate and decreased oxygen saturation.
- Chest X-Ray: initially normal, later shows complications (Putman et al, 1977)
- Arterial Blood Gas: metabolic acidosis, hypoxia, respiratory failure
- Carboxyhaemoglobin: raised levels in CO poisoning
- Bronchoscopy is the most accurate method for diagnosing an inhalational injury. It can also be used as a lavage treatment option.
Classification of Inhalation Injuries
Key Point
An inhalation injury can be supraglottic or subglottic. This anatomical classification reflects different aetiology and expected clinical courses.
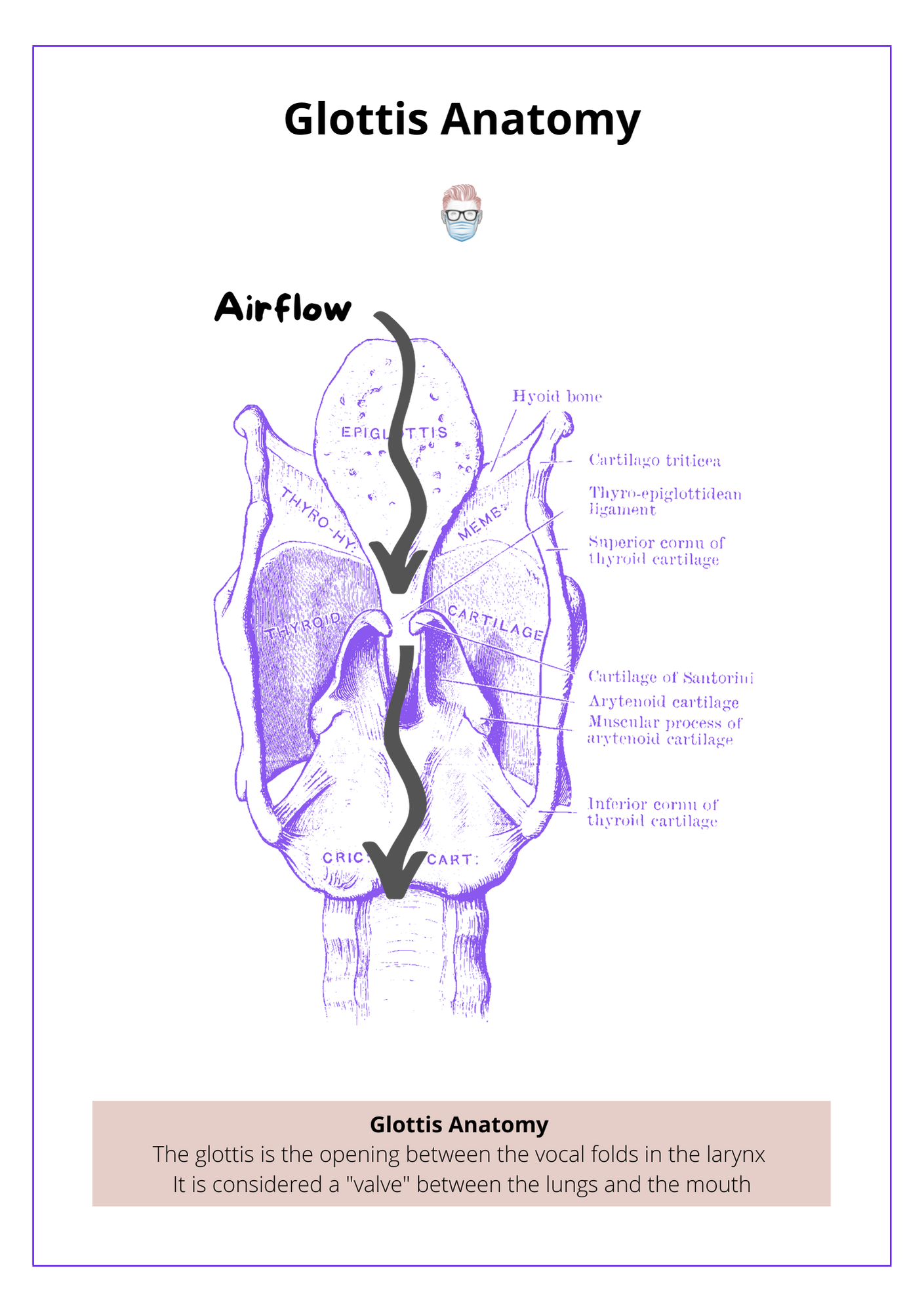
The glottis is the opening between the vocal cords in the larynx. It is a "valve" between the throat and the lungs. This anatomical structure is used as a marker for inhalational injuries. This is illustrated below.
Supraglottic
Direct thermal damage is generally confined to the supraglottic airway.
- Heat is usually the primary cause
- Oedema develops that takes several days to develop
- The airway should be secured
- Exception: steam inhalation is a thermal burn that can travel subglottic.
Subglottic
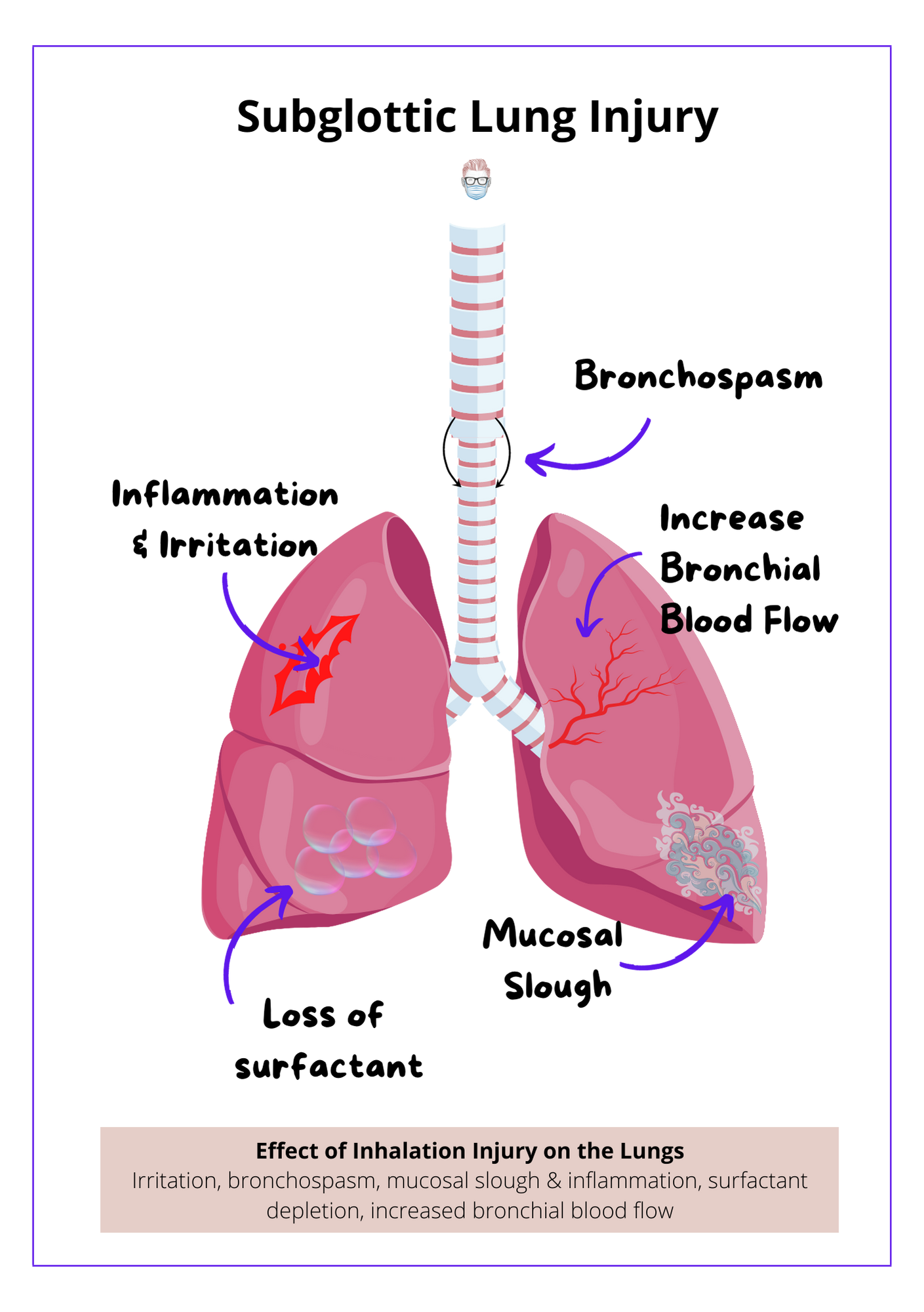
Most injuries that occur below the glottis are caused by aerosolized chemicals and incomplete products of combustion. The various particles result in varying degrees of unpredictability.
- Causes irritation, bronchospasm, mucosal slough and inflammation, surfactant depletion, and increased bronchial blood flow.
- Treated with oxygen, nebulisers, physiotherapy, non-invasive ventilation
- May require intubation for bronchial lavage with sodium bicarbonate.
This is illustrated in the diagram below.
Management of Inhalation Injuries
Key Point
The management of inhalation injuries should focus on airway assessment and patency, medical stabilisation, identifying complications, and respiratory optimisation in a multi-disciplinary team.
Inhalational injuries should be managed as part of a multi-disciplinary team involving plastic surgeons, anaesthetics/critical care, chest physiotherapists, and respiratory doctors.
Goals
The treatment of inhalational injuries is centred on 4 main aspects of care
- Airway support and prevention of therapy-induced lung and airway injury
- Burn Management
- Identifying and treating complications or clinical sequelae.
- Medical optimisation of the patient
Acute Treatment
Burns are trauma and should be treated as per ATLS guidelines. Here are some guidelines specific to the burn only (remember the patient may have other injuries).
- A focused history
- Examine the airway, determine patency or threat to patency
- Examine cutaneous burns and assess for any other injuries
- Perform baseline investigations
- If raised carboxyhemoglobin, 100% high-flow oxygen
- Fluid resuscitation as per Parkland formula if indicated.
Intermediate Treatment
The treatment pathway is time-dependent and should be adjusted to the patient's needs and any complications that may arise. The intermediate treatment often focuses on pulmonary optimisation and clearance. This can be achieved through
- Standard pressure-controlled, lung-protective ventilation strategies.
- Chest physiotherapy
- Bronchoscopy lavage
- Suctioning (if intubated)
- Nebulized heparin and N-acetylcysteine
- Monitoring for infections or respiratory failure
Intubation
Not all inhalation injuries require intubation. It is a case-by-case basis after discussion with critical care/anaesthetic doctors.
Relative indications for intubation include:
- Overt signs of upper-airway obstruction
- Evolving upper-airway obstruction
- Worsening gas of gas exchange
- Obtunded neurologic status
Immediate tracheostomy is rarely necessary. Pulmonary clearance is enhanced by tracheostomy, but this is not a primary indication
Carbon Monoxide Poisoning
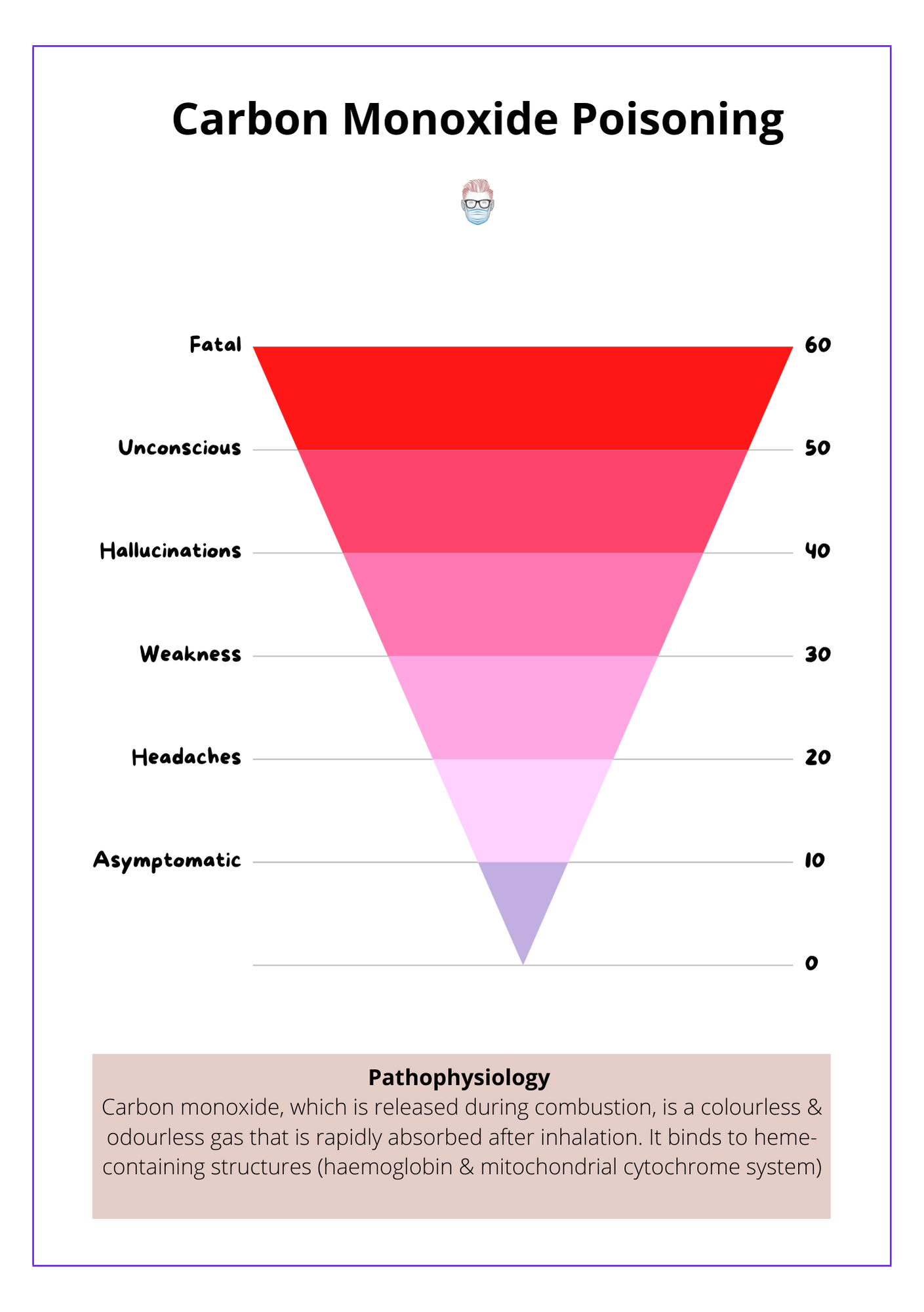
Carbon monoxide, which is released during combustion, is a colourless and odourless gas that is rapidly absorbed after inhalation.
Compared to oxygen, it has ~250x affinity to haemoglobin. This results in oxygen displacement from the haemoglobin.
Pathophysiology
Carbon monoxide binds to heme-containing structures (haemoglobin & mitochondrial cytochrome system). The binding results in:
- Reduced oxygen delivery through the formation of carboxyhemoglobin.
- Reduced oxygen utilization through impaired cytochrome cascade (takes longer to clear)
- The binding of one CO molecule to hemoglobin increases the affinity of the other binding spots for oxygen, leading to a left shift in the dissociation curve
Symptoms
Carbon monoxide can be asymptomatic at low levels. General guidelines for symptoms are listed below
- <20% results in headaches, nausea, confusion
- <30% muscle weakness and impaired cognition
- <40% results in hallucinations and ataxia
- <50% cardiac ischaemia and unconsciousness.
- >60% can be fatal.
Investigations
- Elevated carboxyhaemoglobin (>10% is CO poisoning)
- Metabolic acidosis
- Chest-Xray (usually normal in the acute stages)
- Pulse oximetry cannot differentiate between oxy- and carboxyhaemoglobin because they both absorb light at the same wavelength.
Treatment
- The standard treatment is 100% oxygen for 6 hours (Buckley et al, 2011)
- Monitor metabolic acidosis
Flashcards
They are continually updated and are for thePlasticsPro users.
This is for thePlasticsPro
Join the Club to enjoy unlimited access to all of thePlasticsFella.
Join the Club