

Summary Card
Anatomy of Posterior Interosseous Nerve
Motor branch of the radial nerve
Origin: the radial tunnel at the Arcade of Froshe
Course: between superficial and deep extensors
Innervation: All Extensors except brachioradialis, ERCB, ERCL
Causes of PIN Syndrome
Compression or entrapment is the cause of a Posterior Interosseous Nerve palsy. This compression may be due to trauma, inflammation or iatrogenic.
Clinical Picture of PIN Syndrome
Pain and tenderness is less common than in radial tunnel syndrome
Loss of finger and thumb extension
Wrist extension with radial deviation as ERCL is preserved
No sensory disturbance
Treatment of PIN Syndrome
Non-Surgical: Physiotherapy and Splinting
Surgical: Radial Tunnel Decompression +/- removing cause of compression
Anatomy of Posterior Interosseous Nerve
The Posterior Interosseous Nerve is the motor branch of the radial nerve. This nerve originates at the Arcade of Froshe and travels between the superficial and deep extensors. It innervates all the extensor muscles/tendons except for brachioradialis, ERCB, ERCL.
Origin
The Posterior Interosseous nerve (C7,8) is the motor branch of the radial nerve, which arises in the radial tunnel.
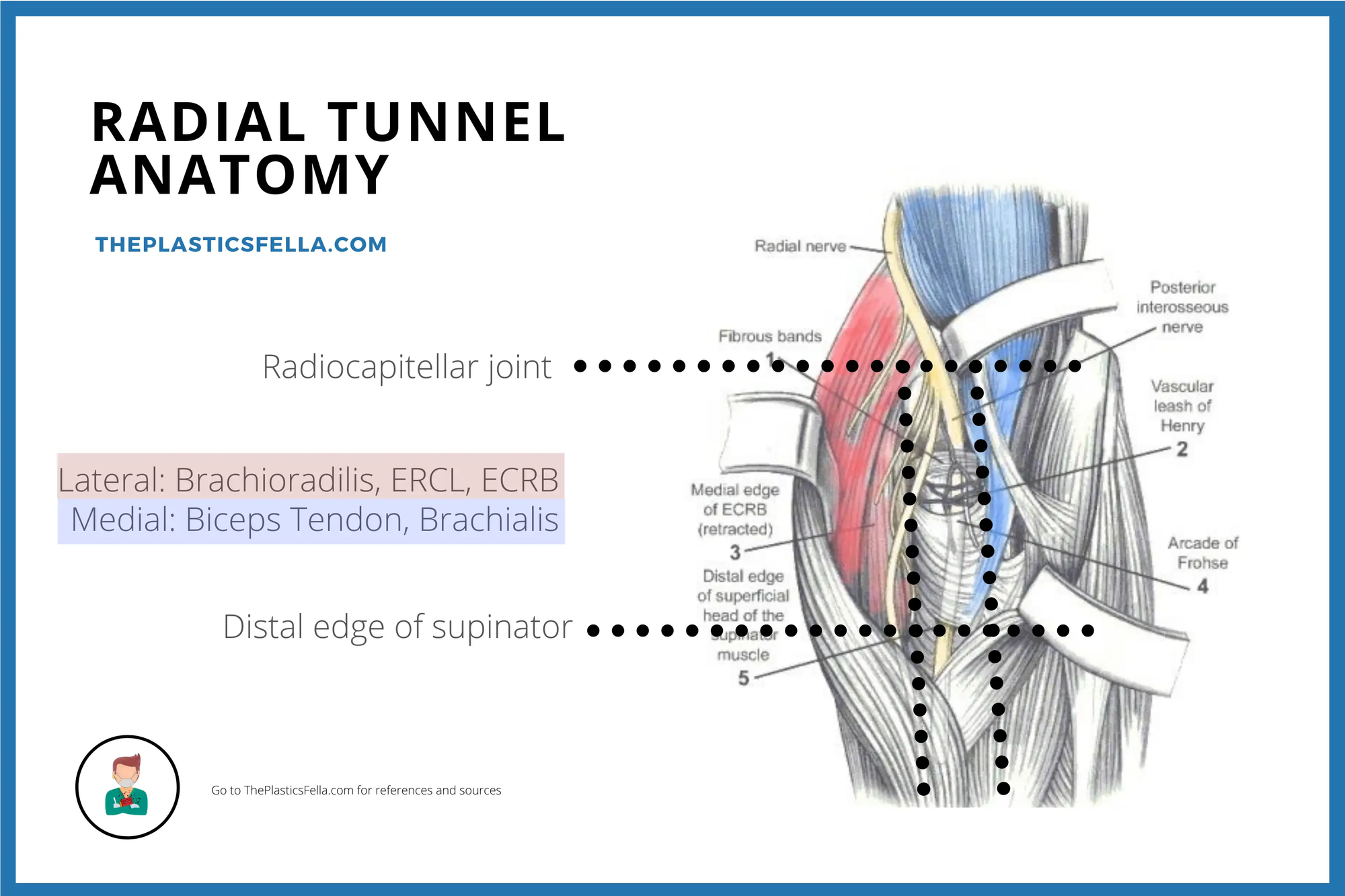
The Radial Tunnel is a 5 cm tunnel from the radiocapitellar joint to the distal edge of the supinator with well-defined anatomical boundaries:
- Lateral: Brachioradialis, ERCL, ECRB
- Medial: Biceps tendon, brachial
- Floor: Capsule of the radiocapitellar joint
This anatomical description can be visualised in the image below:
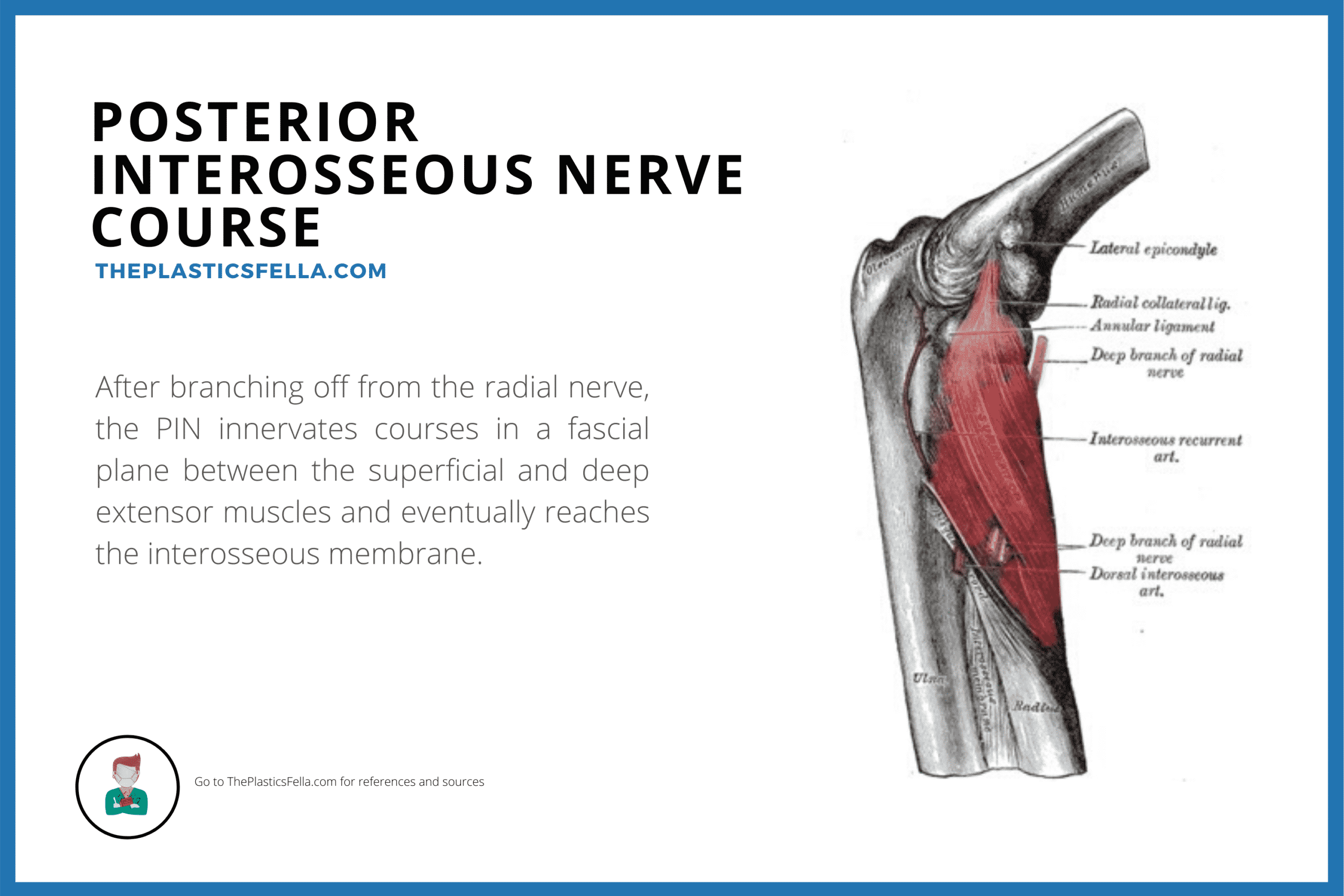
Course
After the Arcade of Froshe, the posterior interosseous nerve travels in a fascial plane between the superficial and deep extensors.
The course of the posterior interosseous nerve is visualised in the image below:
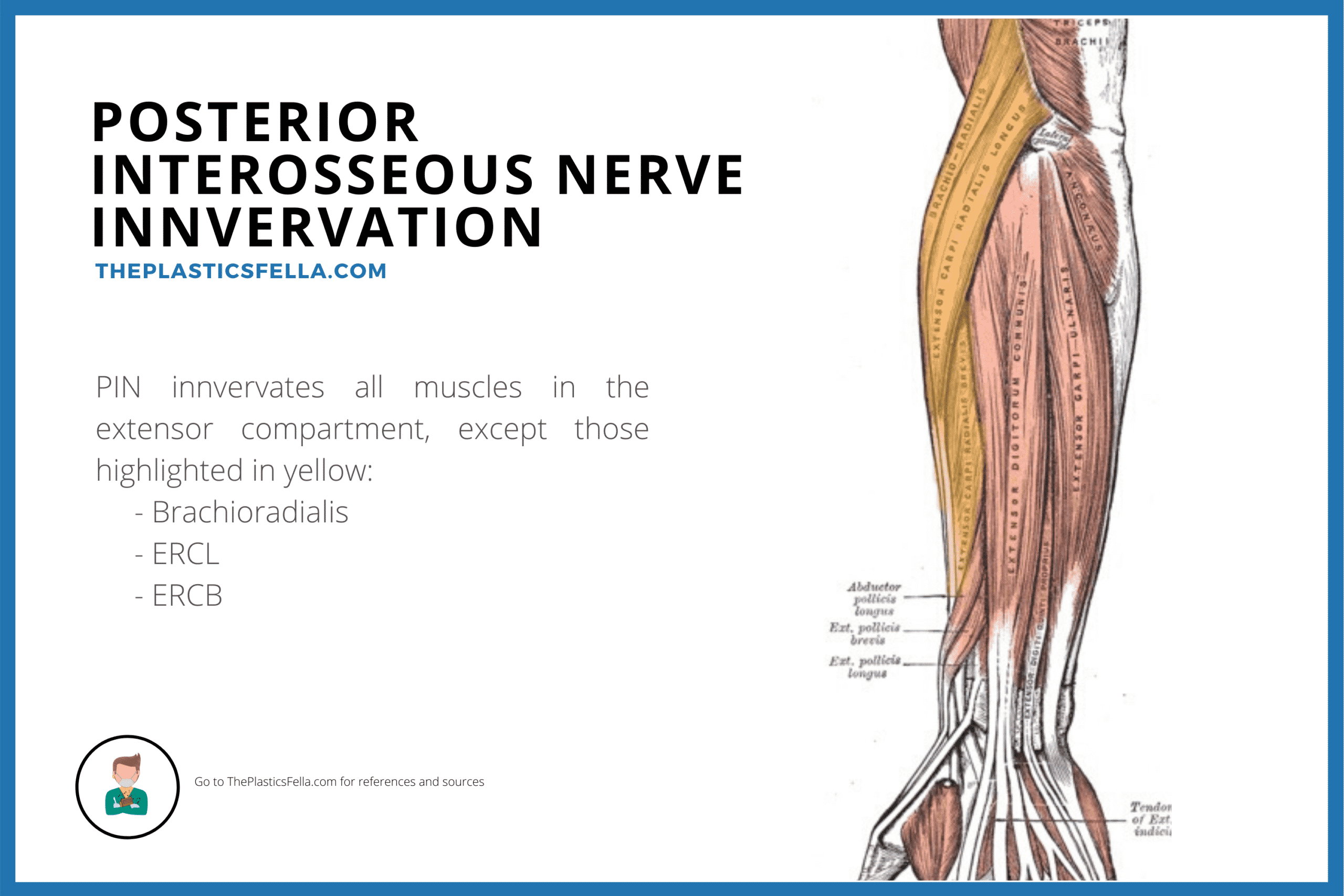
Innervation
The Posterior Interosseous Nerve innervates all forearm extensors apart from ECRL, ECRB and brachioradialis – these muscles are innervated by the radial nerve above the elbow.
This innervation by the Posterior Interosseous nerve is visualise below.
Causes of Posterior Interosseous Syndrome
Posterior Interosseous Nerve syndrome is caused by compression or entrapment. This is commonly due to trauma, inflammation or iatrogenic.
Common Causes of PIN Syndrome/Palsy
The causes of posterior interosseous nerve syndrome/palsy primarily relate to compression. This can be anatomical, pathological or iatrogenic.
| Cause | Example |
|---|---|
| Trauma | Radial Head fracture or dislocation |
| Inflammation | Rheumatoid Synovitis |
| Swelling | Ganglion, Lipomas |
| Iatrogenic | Injections for tennis elbow, plating a radius fracture |
| Anatomical | Common compression site is Arcade of Froshe |
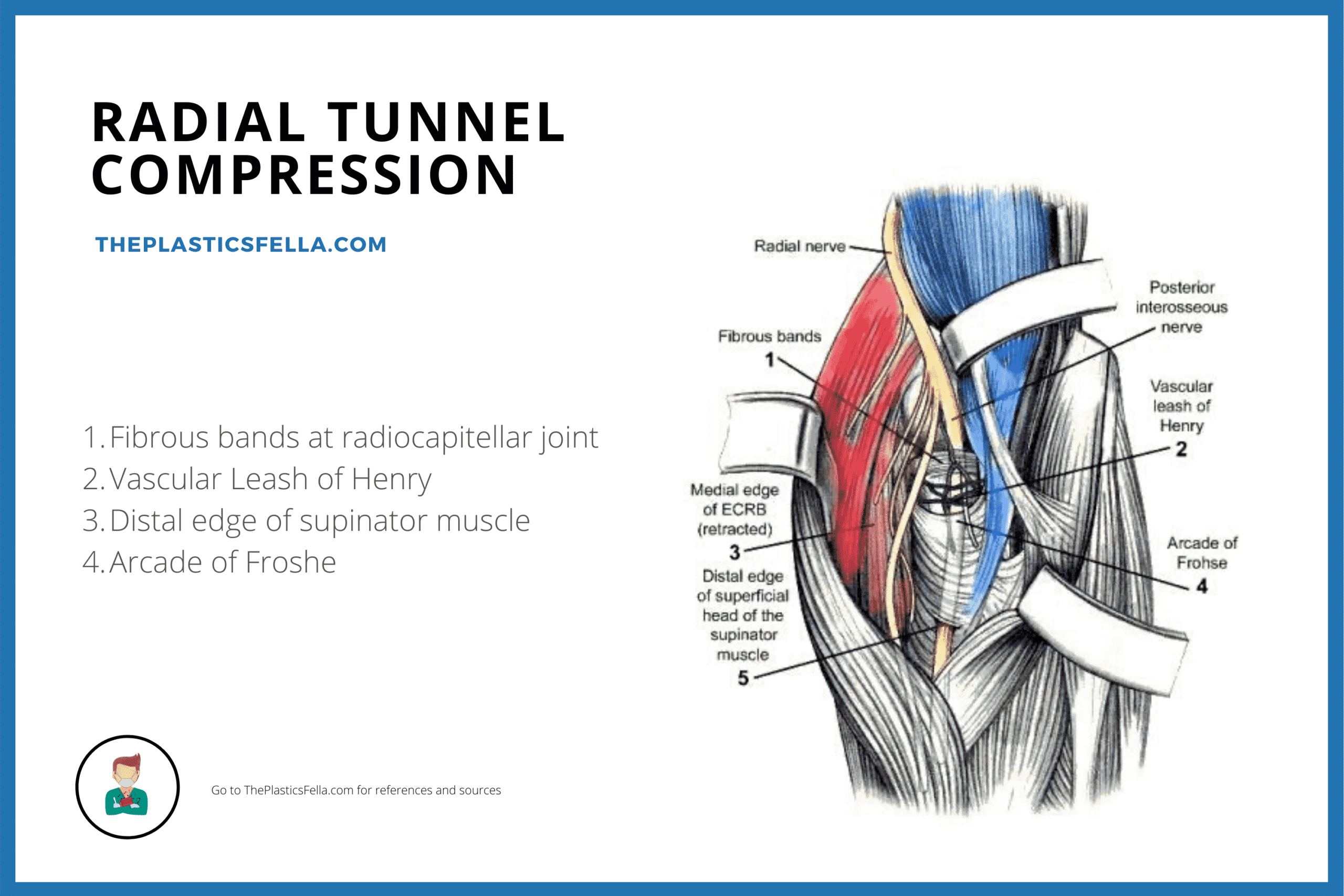
Radial Tunnel Compression Sites
The Posterior Interosseous Nerve is commonly compressed at the Arcade of Froshe. Whilst other compression sites do exist, these occur more proximally and are therefore more relevant to Radial Tunnel Syndrome
The potential compressions are illustrated below:
Diagnosis of Posterior Interosseous Syndrome
Posterior Interosseous Syndrome has motor but no sensory issues. Patients with this palsy have loss of finger and thumb extension, radial deviation on wrist extension (ERCL is preserved). Pain and tenderness is less common than in radial tunnel syndrome.
Function
Posterior Interosseous Nerve (PIN) Palsy presents a unique set of clinical manifestations primarily affecting the motor function of the forearm and hand, with distinct characteristics as follows:
- Difficulty extending the fingers and thumb.
- Wrist extension is spared because ECRL has a more proximal innervation from radial nerve proper.
- Radial deviation with wrist extension may be noted due to ECRB and ECU weakness.
- There is no sensory disturbance
- There may be a Tinel’s Positive Sign
Investigations
To diagnose Posterior Interosseous Nerve (PIN) Palsy Syndrome, the following specific investigations are conducted to assess nerve integrity and identify potential contributing factors:
Nerve Conduction Studies
- In contrast to radial tunnel syndrome, nerve conduction studies is useful
- Fibrillations and denervation potentials in the extensor musculature, are commonly identified.
Imaging
- A case-by-case basis
- Consideration for Ultrasound or MRI if concern for soft tissue mass.
Differential Diagnosis
- Radial Tunnel Syndrome
- Tennis Elbow – Lateral Epicondylitis will have tenderness over lateral epicondyle.
- Attritional Rupture – the presence of a normal tenodesis confirms tendon integrity (passive MPJ extension with wrist flexion
Treatment of Posterior Interosseous Syndrome
Posterior Interosseous Syndrome/Palsy can be treated non-surgically (Physiotherapy and Splinting) and surgically (Radial Tunnel Decompression +/- removing cause of compression).
Non-Surgical
- In the absence of a pathological compression, non-operative measures can be considered a period of up to 3 months before denervation and muscle atrophy.
- Physiotherapy for strength and modify provocative manoeuvres
- Intermittent extension splinting of the MP joints
Surgical Decompression
Generally speaking, surgical decompression is recommended if no recovery after 3 months. A number of different radial tunnel decompression techniques and modifications have been described. The key principles involve:
- Correct any pathological cause of the palsy
- Release Medial border of ERCB
- Release Arcade of Froshe
- Release Leash of Henry
- Superficial head of supinator
This can be performed through different approaches:
- Volar approach between brachioradialis and FCR in the antecubital fossa. This allows good access to proximal sites of compression
- Dorsal approach between ECRL and ECRB or brachioradialis and ECRL. This provides good access to distal sites of compression8.
- Combined approach along the margins of the brachioradialis muscle through a single incision.
Conclusion
Upon completing this article, you will have accomplished the following:
1. Understanding PIN Syndrome: Grasping the clinical presentation of PIN Syndrome as a motor deficit without sensory involvement due to nerve compression.
2. Nerve Anatomy: Becoming familiar with the anatomy and course of the Posterior Interosseous Nerve and its significance in forearm extensor function.
3. Identifying Causes: Identifying common causes of PIN Syndrome, with an emphasis on compression from various sources.
4. Recognizing Symptoms: Differentiating the clinical presentation of PIN Syndrome from similar conditions by focusing on unique motor symptoms.
5. Approaching Treatment: Exploring both non-surgical and surgical treatment options, understanding when each is appropriate based on condition progression.
