

Summary Card
Definition
Ring avulsion injuries occur from sudden traction on a digit, causing damage ranging from circumferential lacerations to complete amputation, with possible vascular compromise.
Mechanisms
Ring avulsion injuries typically occur when rings catch on machinery or stationary objects during everyday activities.
Anatomy
Neurovascular bundle location makes vessels and nerves particularly prone to ring traction injury.
Classification
A circulatory status-based classification such as the Urbaniak classification is useful in guiding treatment options.
Assessment
A thorough assessment should identify all damaged structures, by examining neurovascular status, ROM, and bone injury.
Management
Treatment varies depending on the structures injured ranging from simple suturing and wound care to revascularization, replantation, or amputation of the affected digit.
Primary Contributor: Dr Kurt Lee Chircop, Educational Fellow.
Reviewer: Dr Waruguru Wanjau, Educational Fellow.
Definition of Ring Avulsion Injury
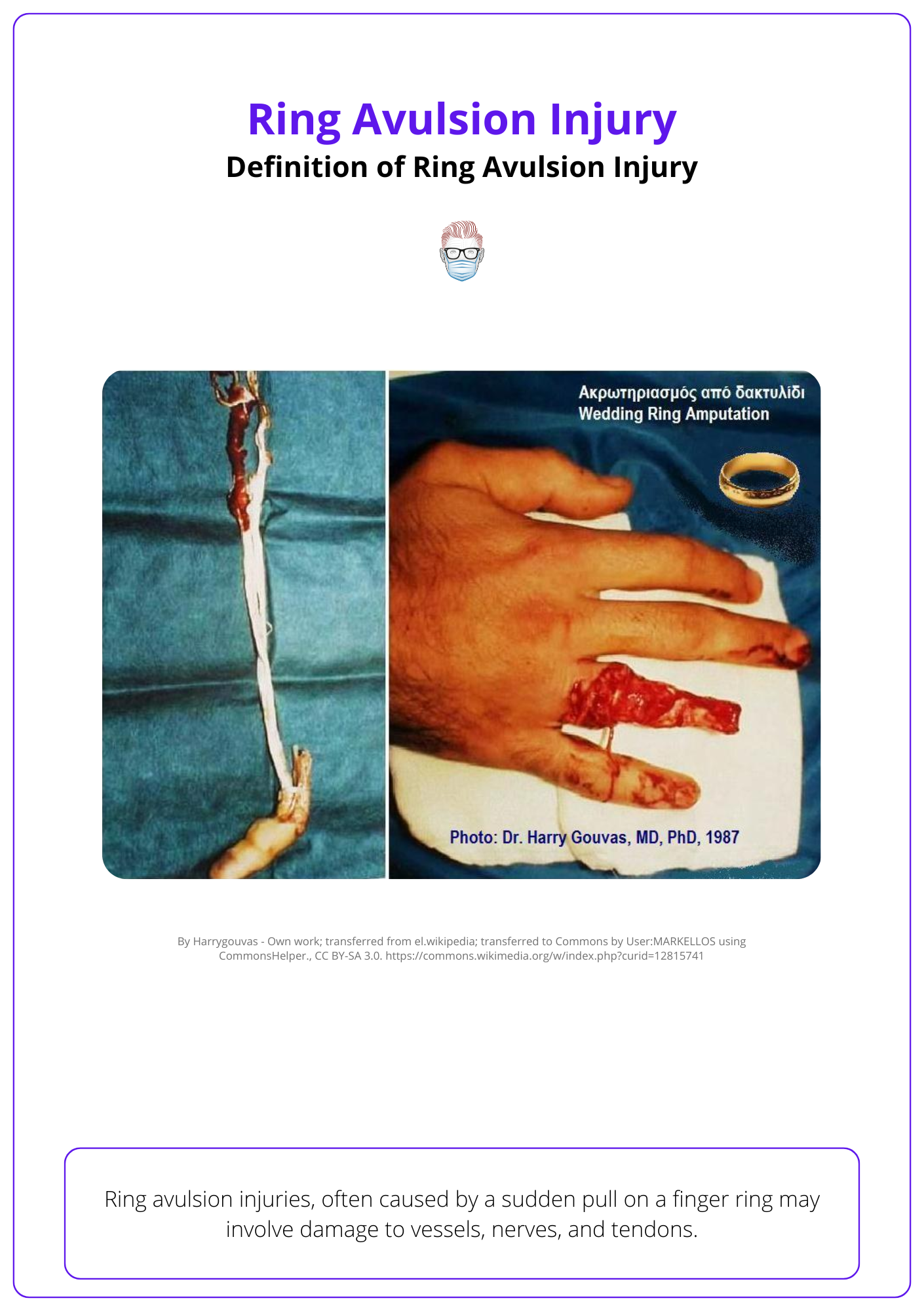
Ring avulsion injuries, often caused by sudden force on a finger ring, can range from lacerations with associated soft tissue injuries to total amputation.
Ring avulsion injuries are typically caused by a sudden pull on a finger ring, resulting in extensive soft tissue damage due to the traction force exerted on the digit.
There is a clinical spectrum of severity dependent on the force of injury. More specifically:
- Skin: ranges from a circumferential laceration to complete finger amputation.
- Associated damage: Injury to vessels, nerves, bone and tendons.
The image below illustrates a Class 3 ring avulsion injury.
Mechanisms of Ring Avulsion Injury
Ring avulsion injuries occur when a ring gets caught, causing forceful traction, with multiple factors affecting the degree of injury.
Ring avulsion injuries happen when a finger ring gets caught on an object, causing a sudden, forceful pull. This can result in various injuries, from minor abrasions to severe degloving or even amputation.
The severity of the injury depends on three main factors,
- Traction Force: A force of 80 newtons can cause injury, additional force associated can cause degloving or complete amputation.
- Duration and Resistance: The length of time and resistance of the ring during the pull also influences the severity of the injury.
- Ring material: Strong alloys are unlikely to buckle from the force applied, leading to more severe injury.
Anatomy of Ring Avulsion Injury
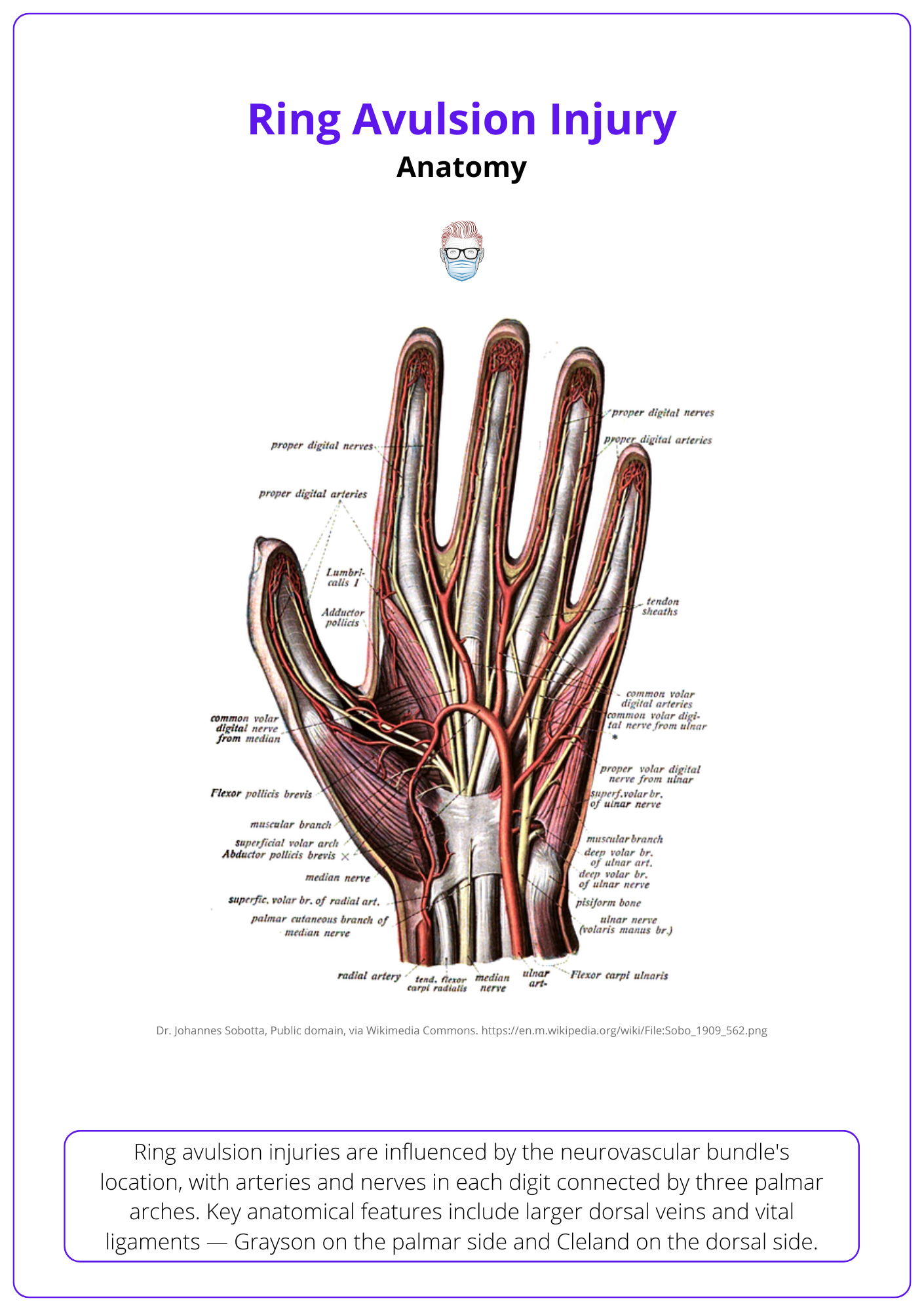
Ring Avulsions can affect bone and soft tissue. In particular, arteries, veins and nerves.
Ring avulsion injuries can affect both soft tissue and bone. In relation to the soft tissue, important anatomical structures to be aware of are the artery and vein.
- Digital Arteries: each digit contains a radial and ulnar digital artery arising from common digital arteries.
- Digital Veins: there is no well defined venous network in the finger. The veins on the dorsal side are larger than those on the palmar side.
- Digital Nerves: each digit contains a radial and ulnar digital nerves arising from common digital nerves.
Neurovascular bundle location makes vessels and nerves particularly prone to ring traction injury. The proper digital arteries communicate with each other at 3 locations: C1 pulley, C3 pulley, FDP insertion.
This is anatomy of the blood supply to the finger is illustrated below.
Urbaniak Classification of Ring Avulsion Injuries
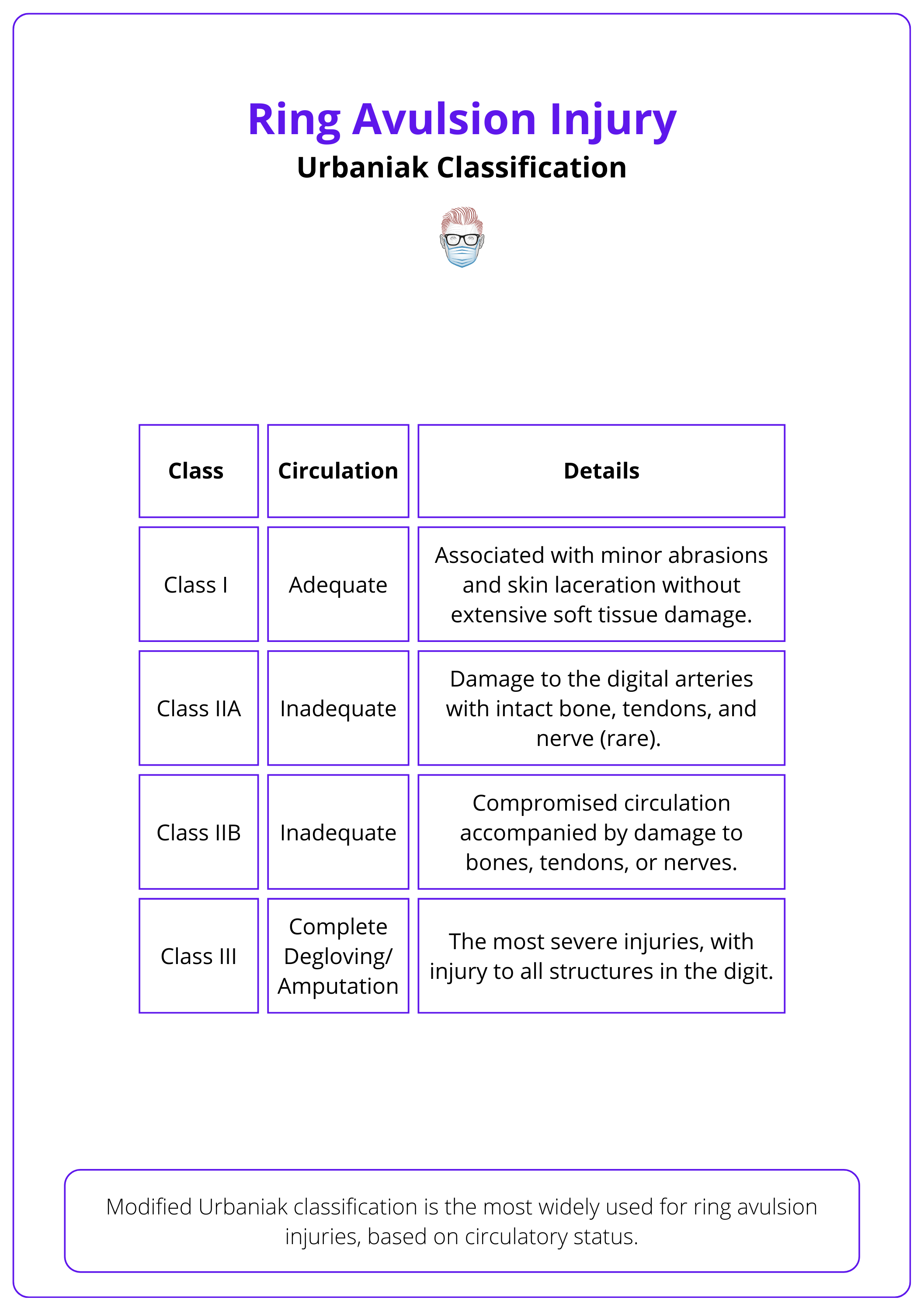
Modified Urbaniak classification is the most widely used, based on circulatory status.
Urbaniak classifies ring avulsion injuries into three categories based on the finger's circulatory status, with Nissenbaum refining Class 2 to reflect skeletal or other soft tissue injuries.
Urbaniak classifies ring avulsion injuries into Class I (Adequate circulation), Class II (inadequate circulation) and class III (complete degloving). This is illustrated in more detail in the table below.
Please note, other classifications exist. These are less commonly used - for exmaple: Kay, Wentz, and Wolf classification (Jones, 2016).
Traditionally, Class III injuries were treated with amputation, but with advancements in microsurgical techniques, successful replantations with satisfactory functional outcomes have been reported (Gardiner, 2021).
Assessment of Ring Avulsion Injuries
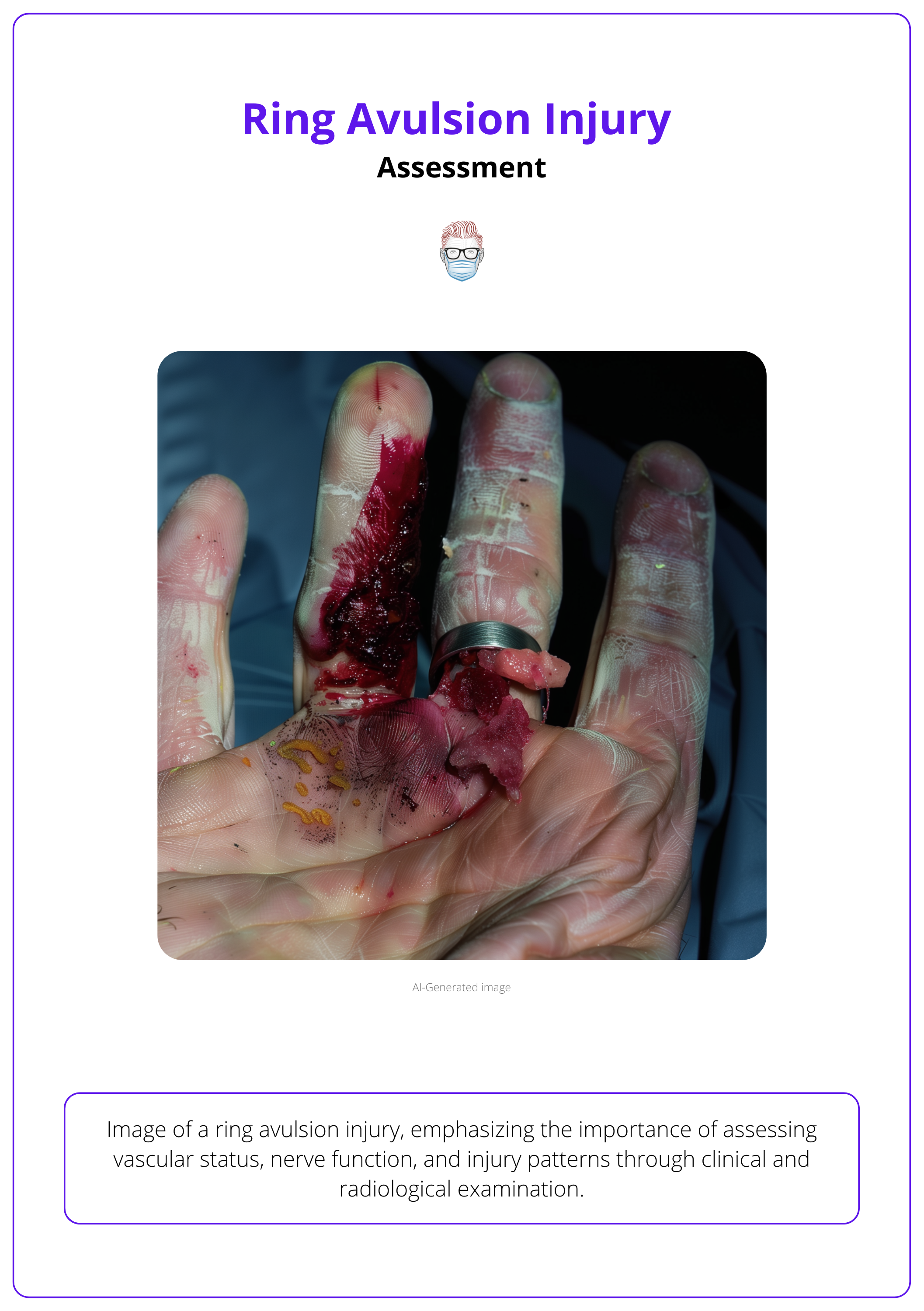
Assess ring avulsion injuries for their vascular status and level of injury. Patient factors should also be considered and supported by radiological investigations.
A thorough examination and classification are vital for determining the appropriate treatment for ring avulsion injuries. The focus should be on these clinical findings:
- Circulation: blood flow to determine vascular damage
- Range of Motion: intact FDS/FDP and extensors
- Nerve Function: degree of sensory disturbance
- Injury Patterns: staggered injury with varying levels of tissue damage
Plain radiographs of the injured digit, including the amputated stump (if available) are useful in identifying the level of injury and any associated fractures.
The image below illustrates a ring avulsion injury.
Digital circulation can be assessed clinically by checking the capillary refill time, or by utilising imaging studies using Doppler US or Hand angiography (Balas, 1980).
Management of Ring Avulsion Injuries
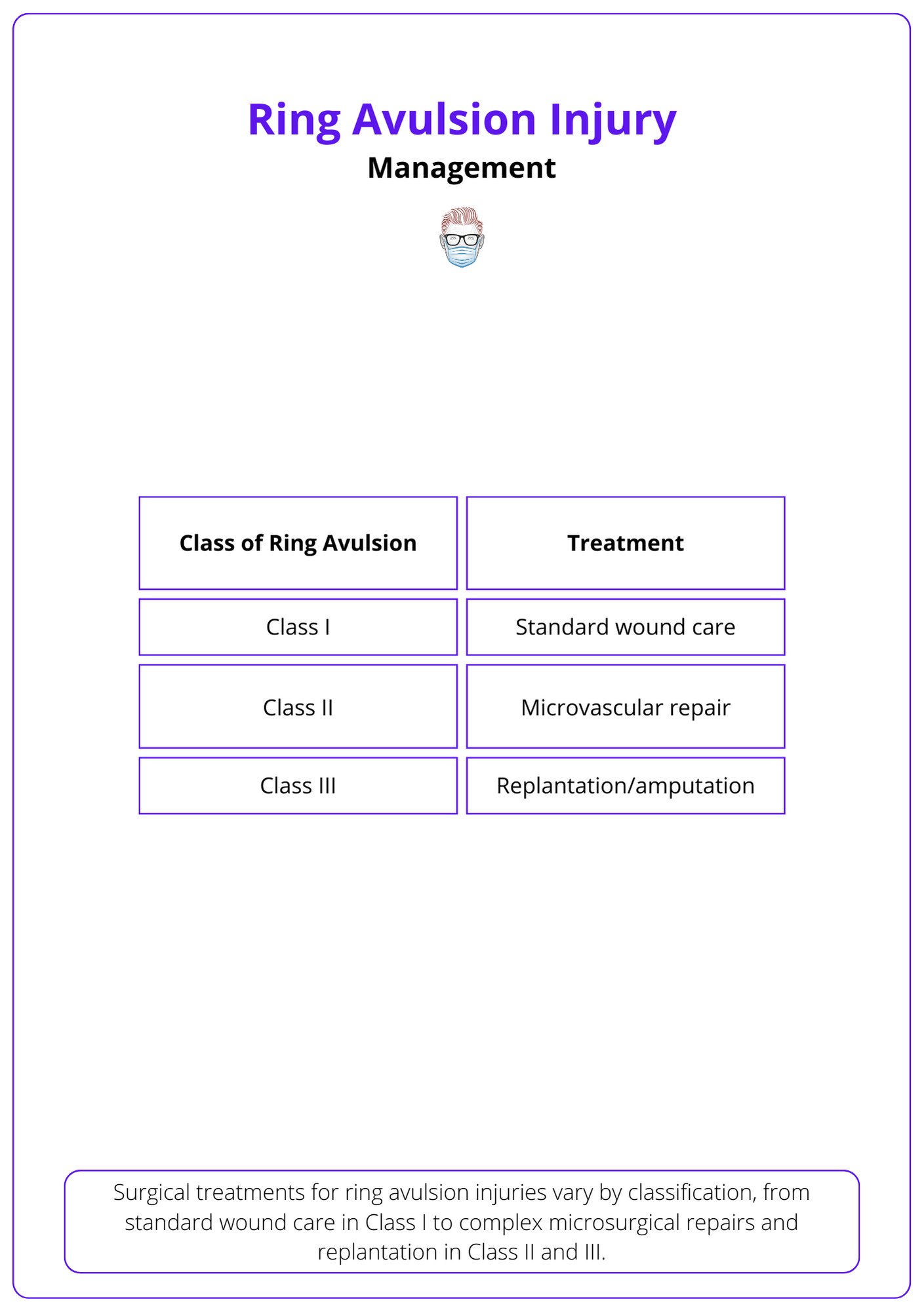
Management is based on severity of injury and involves standard wound care, microsurgical repair, or completion of amputation.
Surgical management of ring avulsion injuries depends on the severity, level of injury, and classification.
Class I Treatment
These patients have adequate circulation without extensive soft tissue damage. These patients should receive:
- Standard wound care
- Delayed skin closure helps prevent constriction and oedema.
- Regular monitoring is critical to detect any signs of deteriorating circulation.
Class II Treatment
These patients have inadequate circulation involving the arteries (IIa) or bones (IIB). These patients should receive
- Microvascular repair: direct end-to-end arterial repair or vein grafts, aiming to repair one artery and two veins.
- Bone Fixation/Tendon reconstruction
- Immobilization to reduce tension on the repairs.
The red line and ribbon signs suggest artery avulsion from a traction injury, indicating that direct repair is inadvisable due to vessel damage. A vein graft is the recommended treatment. (Maricevich, 2011).
Class III Treatment
These patients have complete degloving/amputation.
- Assess suitability for replantation or progress to completion amputation.
- Usually involves vein grafts, venous flaps, and other reconstructive procedures.
Replantation outcomes vary based on the degree of damage, requiring thorough patient counseling and managing expectations (Bamba, 2018).
Below is a summary table of treatment of ring avulsion injuries.
Intimal damage is best assessed under high magnification, allowing resection until healthy vessel tissue is found. The arterial vessel's quality is evaluated with the spurt test. (Gardiner, 2021).
Conclusion
1. Basics of Ring Avulsion Injuries: You have gained a comprehensive understanding of ring avulsion injuries, which occur due to sudden traction on a digit, often from a ring catching on an object, leading to varying degrees of damage from lacerations to amputation.
2. Ring Avulsion Injury Mechanisms: You now understand the mechanisms that contribute to these injuries, including the forces involved and how they can affect the severity of the injury.
3. The Anatomy of Ring Avulsion Injuries: The article provided insights into the specific anatomical structures at risk during a ring avulsion injury, particularly highlighting the vulnerability of the neurovascular bundle and the structural anatomy that can influence the injury outcome.
4. Classification of Ring Avulsion Injuries: You are familiar with the Urbaniak classification system, which is based on circulatory status and helps guide treatment decisions by categorizing the injuries into three main classes.
5. Assessment Techniques of Ring Avulsion Injuries: You've learned about the comprehensive assessment needed for these injuries, including checking neurovascular status, range of motion, and the use of radiographs to understand the extent of damage.
6. Treatment of Ring Avulsion Injuries: Various management strategies for ring avulsion injuries, ranging from conservative treatment with standard wound care to more complex procedures like microsurgical repair, revascularization, replantation, or amputation depending on the severity of the injury.
Further Reading
- Kupfer, David & Eaton, Charles & Swanson, Stephen & Mccarter, M. & Lee, Gilbert. (1999). Ring avulsion injuries: A biomechanical study. The Journal of hand surgery. 24. 1249-53. 10.1053/jhsu.1999.1249.
- Maw, Jonathan, Kai Yuen Wong, and Patrick Gillespie. "Hand anatomy." British Journal of Hospital Medicine 77.3 (2016): C34-C40. https://doi.org/10.12968/hmed.2016.77.3.C34
- Jones M, Gujral S. Ring Avulsion Injuries. Eplasty. 2016 Feb 10;16:ic5. PMID: 26933469; PMCID: PMC4753839.
- Gardiner S, Friebel TR, Bray J, Anadkat M, Nikkhah D. Practical Techniques to Ensure Success in Digital Ring Avulsion Injuries. Plast Reconstr Surg Glob Open. 2021 Aug 19;9(8):e3771. doi: 10.1097/GOX.0000000000003771. PMID: 34667701; PMCID: PMC8517313.
- Balas P, Katsogiannis A, Katsiotis P, Karaitianos J. Comparative study of evaluation of digital arterial circulation by doppler ultrasonic tracing and hand arteriography. J Cardiovasc Surg (Torino). 1980 Jul-Aug;21(4):455-62. PMID: 7419562.
- Bamba R, Malhotra G, Bueno RA Jr, Thayer WP, Shack RB. Ring Avulsion Injuries: A Systematic Review. Hand (N Y). 2018 Jan;13(1):15-22. doi: 10.1177/1558944717692094. Epub 2017 Feb 16. PMID: 28720047; PMCID: PMC5755869.
- Maricevich M, Carlsen B, Mardini S, Moran S. Upper extremity and digital replantation. Hand (N Y). 2011 Dec;6(4):356-63. doi: 10.1007/s11552-011-9353-5. Epub 2011 Aug 4. PMID: 23204960; PMCID: PMC3213257.
