

Summary Card
Scaphoid Bone Anatomy
The scaphoid has three regions: proximal pole, waist (corresponding to the anatomical snuffbox), and distal pole.
Scaphoid Ligament Anatomy
Key ligaments include Scapholunate Interosseous and Radioscaphocapitate, with volar ligaments being stronger.
Blood Supply to the Scaphoid
Radial artery provides 70-80% of blood supply. Dorsal blood enters via dorsal ridge foraminae; volar supply is 20-30% of internal vascularity, mainly in the distal pole.
Imaging the Scaphoid Anatomy
Multiple angles needed, including PA view in ulnar deviation, 60° pronation, and 60° supination. Lateral view detects DISI or VISI deformities.
Scaphoid Bone Anatomy
The scaphoid has a proximal pole, waist, distal pole. Unique curvatures and angles allows articulation to radial, lunate, trapezoid, and trapezium bones.
Anatomical Regions
The scaphoid forms a mechanical linkage between the carpal rows. It serves as the lateral column in the proximal carpal row arch and can be divided into three basic regions:
- Proximal pole
- Waist
- Distal pole
The below video visalizes the anatomy of scaphoid bone.
Scaphoid Bone Anatomy
It possesses both a palmar concave and medial (ulnar) concave curvature. The angle from the proximal to distal pole (ie the intrascaphoid angle) is 40°± 3° in the coronal plane and 32°± 5° in the sagittal plane (Berger, 2001).
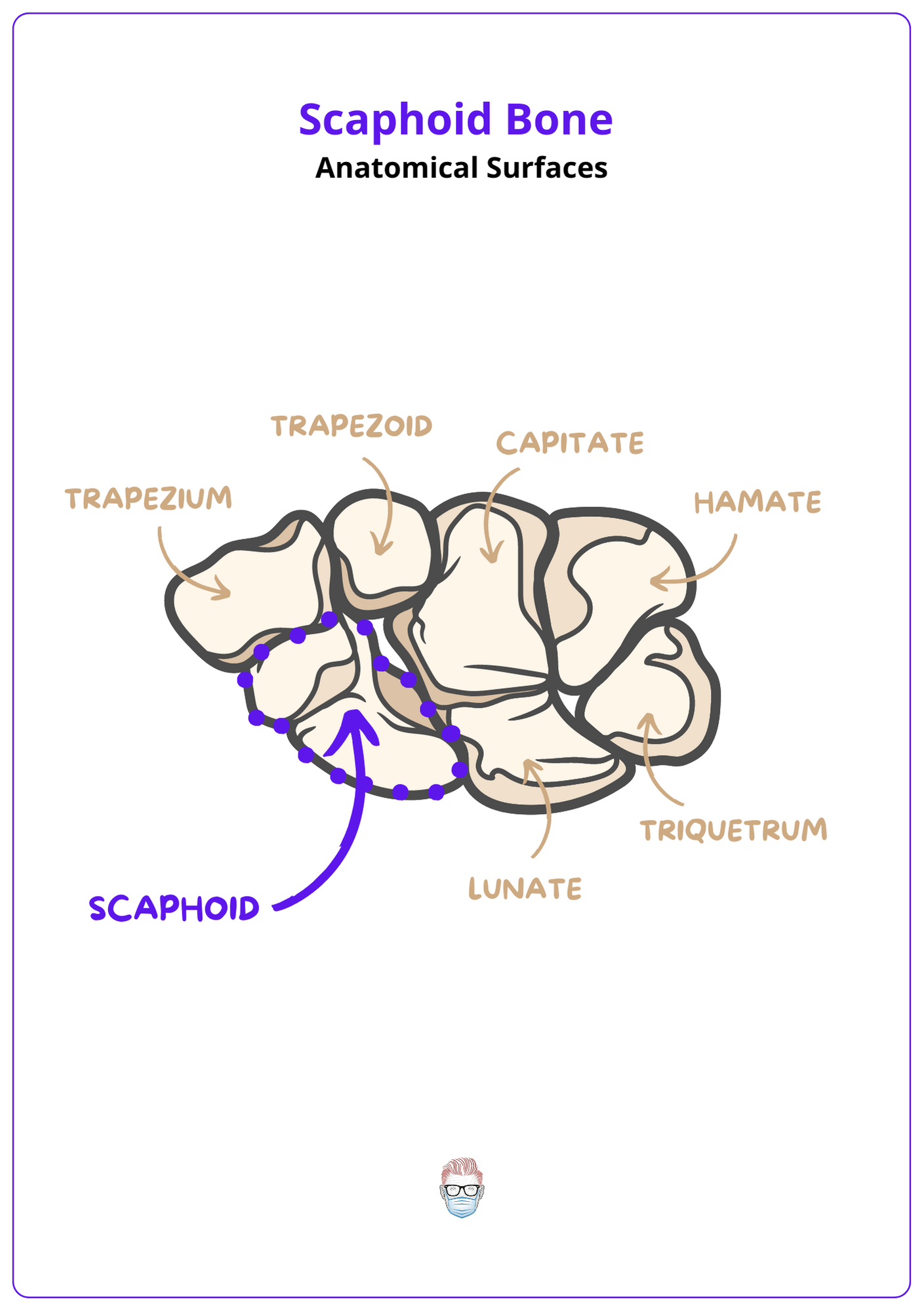
Anatomical Surfaces
The scaphoid's surfaces are often described as proximal, lateral, distal, and medial surfaces. Each surface has a specific feature and articulation.
- Proximal surface: hemispheric, articulates with scaphoid fossa of radius.
- Medial surface: flat and crescentic, articulates with the lateral lunate surface
- Distal surface: slightly convex, articulates with the trapezoid and trapezium.
This scaphoid anatomy is described in the image below.
Scaphoid Ligament Anatomy
The scaphoid's ligaments, including the Scapholunate Interosseous, Radioscapholunate, Radioscaphocapitate, and Scaphotrapezium Ligaments, play a critical role in the stability of fractured fragments, with the carpal capsule being reinforced by stiffer volar ligaments.
The scaphoid's fracture serves to highlight the importance of its ligaments, which govern the stability of the fractured fragments. The carpal capsule receives reinforcement from both dorsal and volar ligaments, with the volar ligaments being notably stronger. Some ligaments to mention include:
- Scapholunate: C-shaped structure connecting the scaphoid and lunate bones, with a thicker dorsal fiber that provides the primary constraint to their translation, while its proximal fibers possess minimal mechanical strength.
- Radioscapholunate: "ligament of Testut and Kuentz" is not a true ligament, functioning only as a neurovascular conduit without adding mechanical strength.
- Radioscaphocapitate: ligament from the radial styloid to the capitate acts as a sling to support the waist of the scaphoid.
This image visualizes ligament anatomy as discussed above.

The scaphoid is also acted on by flexor and extensor tendons. More specifically:
- Flexor Carpi Radialis Tendon: a fibro-osseous tunnel on its distal pole.
- Extensor Carpi Radialis Brevis and Longus: bolster the posterior wrist joint capsule covering the scaphoid.
The scaphoid serves as a focus of ligamentous attachment and represents one of two areas in the proximal carpal row, the other being the pisiform, that are dynamically influenced by extrinsic musculotendinous structures.
Blood Supply to the Scaphoid
The scaphoid primarily receives blood from the radial artery, accounting for 70-80% of its intraosseous supply, with vessels accessing both externally via dorsal and volar routes and internally, chiefly through dorsal ridge foraminae.
The scaphoid's vascular supply is predominantly retrograde, intricately moving from distal to proximal. It primarily receives its blood supply from the radial artery (70-80%), which further bifurcates into the dorsal carpal branch and the superficial palmar/volar branch. These vessels enter the scaphoid through distal half of the bone.
Dorsal carpal branch
- Supplies ~70%, especially its distal two-thirds.
- Enters via the foramina on the dorsum oblique ridged between the articular surfaces for the radius and for the trapezium and trapezoid.
Superficial palmar/volar branch
- Supplies ~30%, especially the distal tuberosity.
- Enters via the tubercle, which is concave volar aspected with a rounded elevation.
Gelberman's landmark paper in the 1980s showed:
- The ulnar artery doesn't contribute to the scaphoid's vascularity.
- The anterior interosseous artery makes a significant contribution.
- There are no significant intra-osseous anastomoses between the dorsal and volar branches of the scaphoid, a result of the scaphoid emerging from the fusion of two chondrification zones.
Imaging the Scaphoid Anatomy
Multiple imaging angles, including PA view in ulnar deviation, 60° pronation, and 60° supination, are essential for the scaphoid's detailed assessment, while the lateral view helps detect DISI or VISI deformities.
The scaphoid's complex anatomy demands multifaceted imaging for a comprehensive assessment. More than two views are required due to its intricate shape and alignment.
PA View in Ulnar Deviation:
- This extends the scaphoid to provide a clear image of all scaphoid regions.
- Minimal overlap of adjacent bones.
Oblique View
- 60° Pronation: focuses the distal pole and tubercle.
- 60° Supination: focuses the scaphoid's proximal pole.
Lateral View:
- A difficult view to assess the scaphoid itself due to overlapping structures.
- Useful for assess any DISI or VISI deformity.
Conclusion
1. Scaphoid Anatomy: Acquired detailed insights on the scaphoid bone's structure, including its three distinct regions (proximal pole, waist, and distal pole), and its unique curvatures and angles that allow for articulation with surrounding carpal and radial bones.
2. Ligament Anatomy: Learned about key ligaments associated with the scaphoid, such as the Scapholunate Interosseous and Radioscaphocapitate ligaments, and their significance in maintaining the stability of the wrist and scaphoid fractures.
3. Vascular Anatomy of the Scaphoid: Gained an understanding of the scaphoid's blood supply, predominantly from the radial artery, and how its unique vascular anatomy influences healing and the risk of avascular necrosis.
4. Imaging in Scaphoid Evaluation: Explored the critical role of various imaging techniques, including PA views in ulnar deviation, pronation, and supination, in diagnosing scaphoid fractures and assessing anatomical details crucial for treatment planning.
Further Reading
- Berger RA. The gross and histologic anatomy of the scapholunate interosseous ligament. J Hand Surg [Am]. 1996;21:170-178.
- Berger RA, Landsmeer JMF. The palmar radiocarpal ligaments: A study of adult and fetal human wrist joints. J Hand Surg [Am]. 1990;15:847-854.
- Berger RA, Crowninshield RD, Flatt AE. The three-dimensional rotational behaviors of the carpal bones. Clin Orthop Rel Res. 1982;167:303-310.
- Bettinger PC, Linscheid RL, Berger RA, et al. An anatomic study of the stabilizing ligaments of the trapezium and trapeziometacarpal joint. J Hand Surg [Am]. 1999;24:786-798.
- Gelberman RH, Menon J. The vascularity of the scaphoid bone. J Hand Surg. 1980;5:508-513.
- Gelberman RB, Panagis JS, Taleisnik J, et al. The arterial anatomy of the human carpus. Part I. The extraosseous vascularity. J Hand Surg [Am]. 1983;8:367-375.
- Kobayashi M, Berger RA, Linscheid RL, et al. Intercarpal kinematics during wrist motion. Hand Clin. 1997;13:143-149.
- Kobayashi M, Berger RA, Nagy L, et al. Normal kinematics of carpal bones: A three-dimensional analysis of carpal bone motion relative to the radius. J Biomech. 1997;30:787-793.
- Panagis JS, Gelberman RB, Taleisnik J, et al. The arterial anatomy of the human carpus. Part II: The intraosseous vascularity. J Hand Surg [Am]. 1983;8:375-382.
- Smith DK, Linscheid RL, Amadio PC, et al. Scaphoid anatomy: Evaluation with complex motion tomography. Radiology. 1989;173:177-180.
- Taleisnik J, Kelly PJ. The extraosseous and intraosseous blood supply of the scaphoid bone. J Bone Joint Surg [Am]. 1966;48:1125-1137.
- Viegas SF, Yamaguchi S, Boyd NL, et al. The dorsal ligaments of the wrist: Anatomy, mechanical properties, and function. J Hand Surg [Am]. 1999;24:456-468.
- Cave EF. The carpus with reference to fractured navicular bone. Arch Surg. 1940;40:54-76.
- Mazet R Jr, et al. Fractures of the carpal navicular, analysis of 91 cases and review of the literature. J Bone Joint Surg [Am]. 1963;45:82-112.
- Rockwood CA, et al. Fractures, vol 1. Philadelphia: JB Lippincott Co; 1975.
- Barber H. The intraosseous arterial anatomy of the adult human carpus, in Orthopedics, vol 5. Oxford: Donald Parson; 1972. p. 20.
- Grettve S. Arterial anatomy of the carpal bones. Acta Anat (Scand). 1955-6;25:331-45.
- Lutzeler H. Die entstehungsursache der pseudarthrose nach bruch des kahnbeins der hand. Dtsch Z Chir. 1932;235:450-67.
- Travaglini F. Arterial circulation of the carpal bones. Bull Hosp Joint Dis NY. 1959;20:19-36.
- Obletz BE, et al. Non-union of fractures of the carpal navicular. J Bone Joint Surg [Am]. 1938;20:424-8.
- Russe O. Fracture of the carpal navicular: diagnosis, non-operative treatment, and operative treatment. J Bone Joint Surg [Am]. 1960;42:759-68.
- Bohler L. The treatment of fractures, vol 1. New York: Grune & Stratton, Inc; 1956.
- Roolker W, Maas M, Broekhuizen AH. Diagnosis and treatment of scaphoid fractures, can non-union be prevented. Arch Orthop Trauma Surg. 1999;119(7–8):428–31.
- Trojan E. Der Kahnbeinbruch der Hand. In: Habilitationschrift. Wien: Eigenverlag & Bruck Bru ̈der Hollinek; 1961.
- Zolczer L, Glanz J. A sajkacsontto ̈re ́s. In: A ke ́zto ̋ fedett se ́ru ̈le ́sei, elva ́ltoza ́sai. Budapest: Medicina; 1995.
- Roolker L, Tiel-van Buul MM, Bossuyt PP, Dijkstra PF, van Grieken HJ, Broekhuizen TH. The value of additional carpal box radiographs in suspected scaphoid fracture. Invest Radiol. 1997;32(3):149–53.
- Roolker W, Tiel-van Buul MM, Bossuyt PM, et al. Carpal Box radiography in suspected scaphoid fracture. J Bone Joint Surg [Br]. 1996;78(4):535–9.
- Roolker W, Tiel-van Buul MM, Ritt MJ, Verbeeten Jr B, Griffioen FM, Broekhuizen AH. Experimental evaluation of scaphoid X-series, carpal box radiographs, planar tomography, computed tomography and magnetic resonance imaging in the diagnosis of scaphoid fracture. J Trauma. 1997;42(2):247–53.
- Tiel-van Buul MM, van Beek EJ, Broekhuizen AH, Nooitgedacht EA, Davids PH, Bakker AJ. Diagnosing scaphoid fractures: radiographs cannot be used as a gold standard! Injury. 1992;23(2):77–9.
- Tiel-van Buul MM, van Beek EJ, Dijkstra PF, Bakker AD, Griffioen FM, Broekhuizen TH. Radiography of the carpal scaphoid. Experimental evaluation of “the carpal box” and first clinical results. Invest Radiol. 1992;27(11):954–9.
