

Summary Card
UCL Anatomy of the Thumb
The ulnar collateral ligaments is a thumb MCPJ stabiliser. It is most commonly injured following forced abduction.
Aetiology
UCL injuries can be acute (“Skier’s thumb”) or chronic (“Gamekeeper’s thumb”).
Assessment
Pain, swelling, and bruising, diagnosed with valgus stress tests. Imaging to bony involvement and MCPJ arthritis.
Management
Conservative methods for acute partial tears. Surgery (repair, reinforce, or reconstruct) for complete tears, chronic, Stener Lesion.
Primary Contributor: Dr Suzanne Thomson, Educational Fellow.
Reviewer: Dr Kurt Lee Chircop, Educational Fellow.
UCL Anatomy of the Thumb
The UCL provides stability to the thumb MCPJ, particularly to valgus stress/radial deviation. The joint is also supported by radial collateral ligaments, volar plate, sesamoid bones, and flexor tendons.
The ulnar collateral ligament (UCL) runs obliquely from the lateral condyles of the metacarpal to insert on the volar distal phalanx. This dorsal-volar course enables this structure to be taut in flexion and loose in extension.
The UCL anatomy can be visualised below.
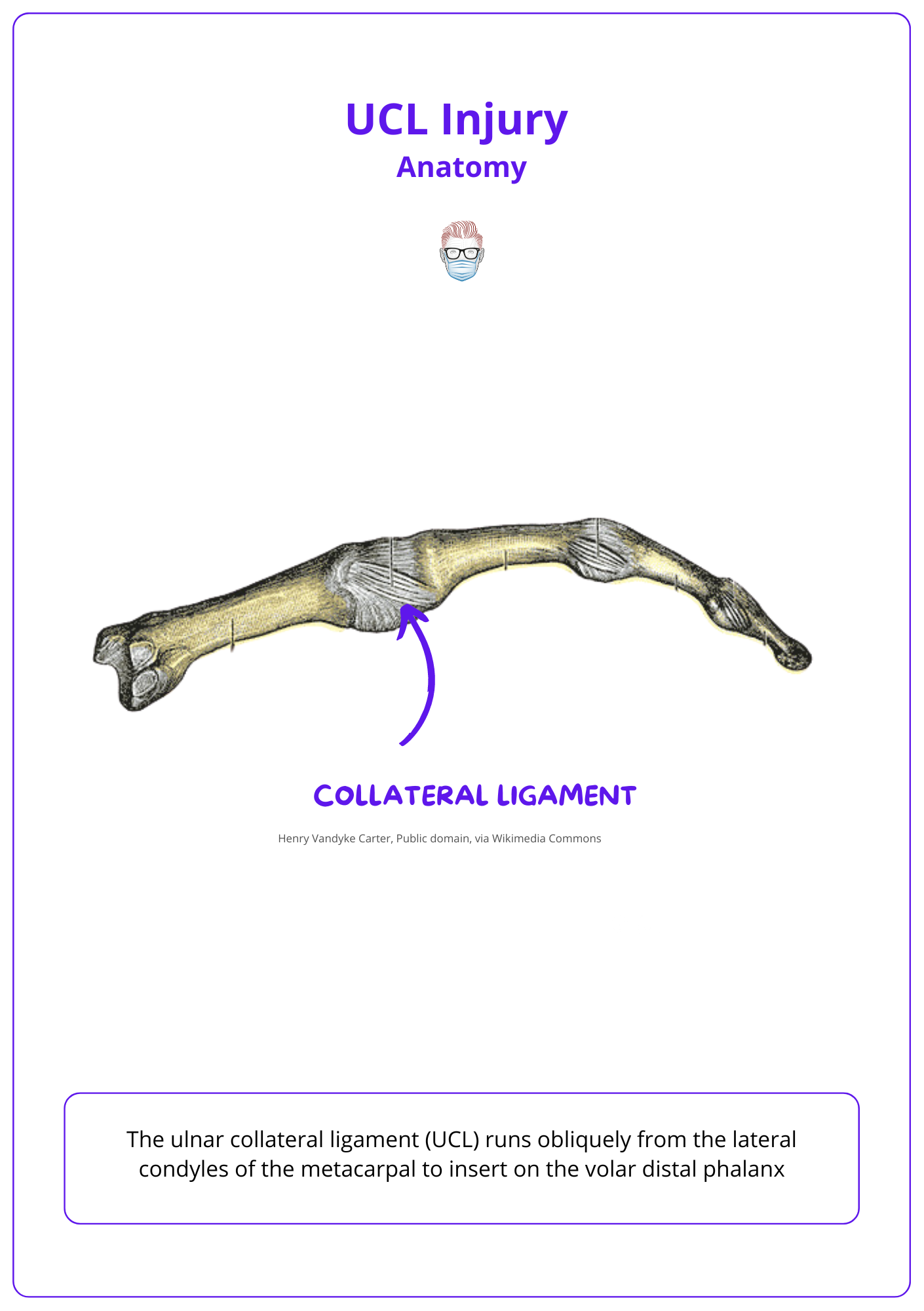
The thumb MCPJ is a condyloid joint that relies predominantly on the strong ulnar and radial collateral ligaments for stability. Further stability is provided by:
- Accessory collateral ligaments
- Volar plate
- Sesamoid bones
- Flexor tendons.
The ulnar collateral ligament is a thick band approximately, 4-8mm wide 12-14mm long.
Aetiology of Thumb MCPJ UCL Injury
Acute ulnar collateral ligament injuries of the thumb are common in skiers and often involve avulsion fractures. These are typically managed based on injury severity, with surgery recommended for severe cases.
Acute UCL Injury
Acute ulnar collateral ligament injuries are caused by forced radial abduction of the thumb. They are more common than radial collateral injuries and often seen in skiers.
An UCL injury may be associated with an avulsion fracture. Many fracture patterns exist but important points are:
- It can occur at ulnar base of the proximal phalanx
- The size of the avulsion fracture has been used to guide management; with a fragment >2mm being used as an indication for surgery
Chronic
Chronic UCL injuries are commonly referred to as Gamekeeper's thumb due to the chronic stretching of the UCL after repeated abduction movements.
This was described by Scottish surgeon, Campbell, in gamekeepers who broke rabbits necks between their thumb and index finger, the force being transmitted over a fulcrum formed by the ulnar aspect of their thumb.
Assessment of Thumb MCPJ UCL Injury
Thumb MCPJ UCL injuries, characterized by pain, swelling, and bruising from forced abduction, require valgus stress tests and imaging to assess ligament damage.
The diagnosis a thumb MCPJ UCL injury requires clinical and radiological investigations.
In terms of the patient's history, common findings include:
- History of forced abduction accompanied
- Pain, bruising, and swelling at the base of the thumb
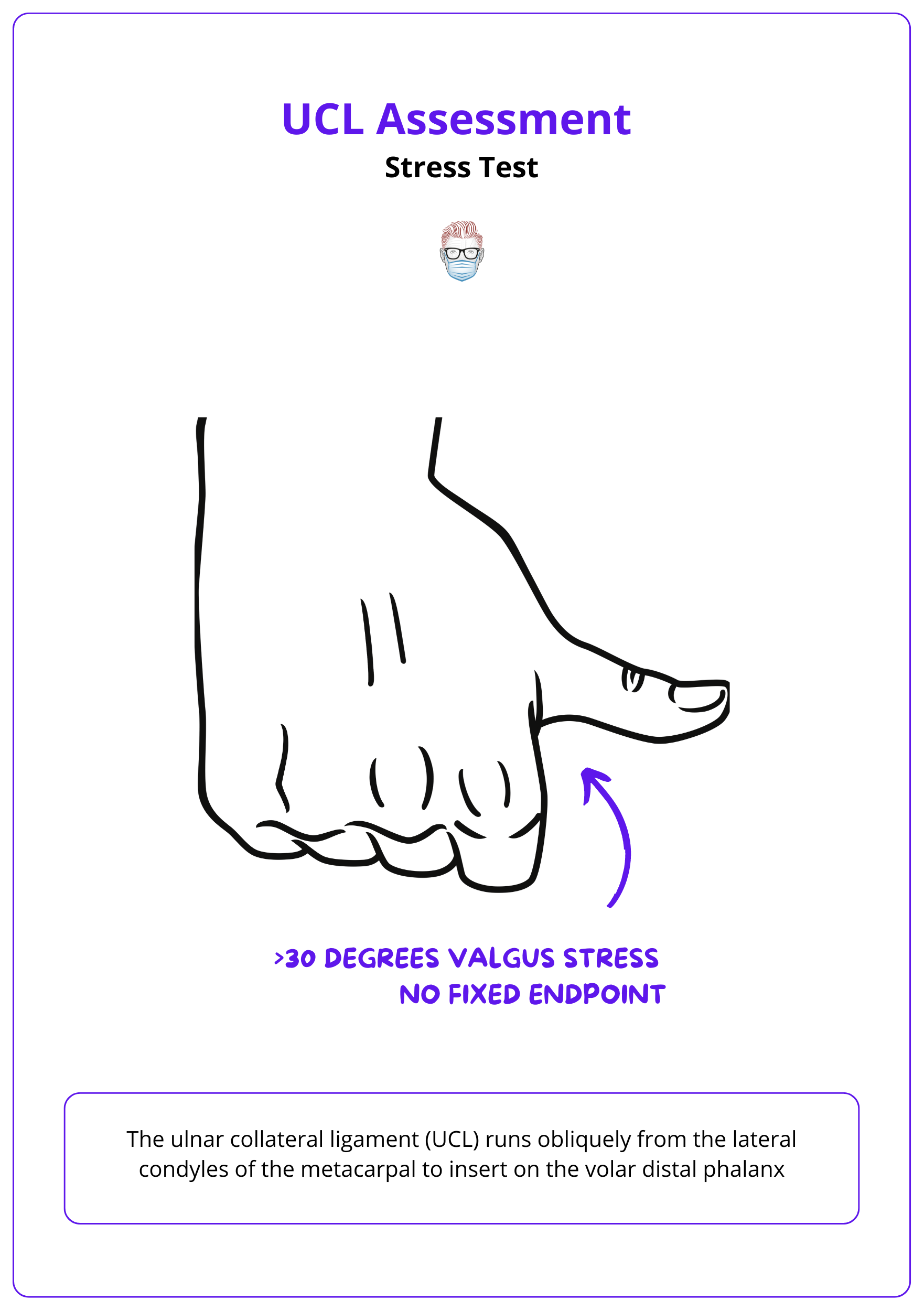
In relation to clinical examination, common findings include:
- Weakness of pinch grip.
- Increase angle on valgus stress of the MCPJ: 30 degrees or >15% compared the other hand (Avery, 2015).
- Discrete (partial) or loss of endpoint (complete) on valgus stress.
Classification of MCPJ UCL Injuries
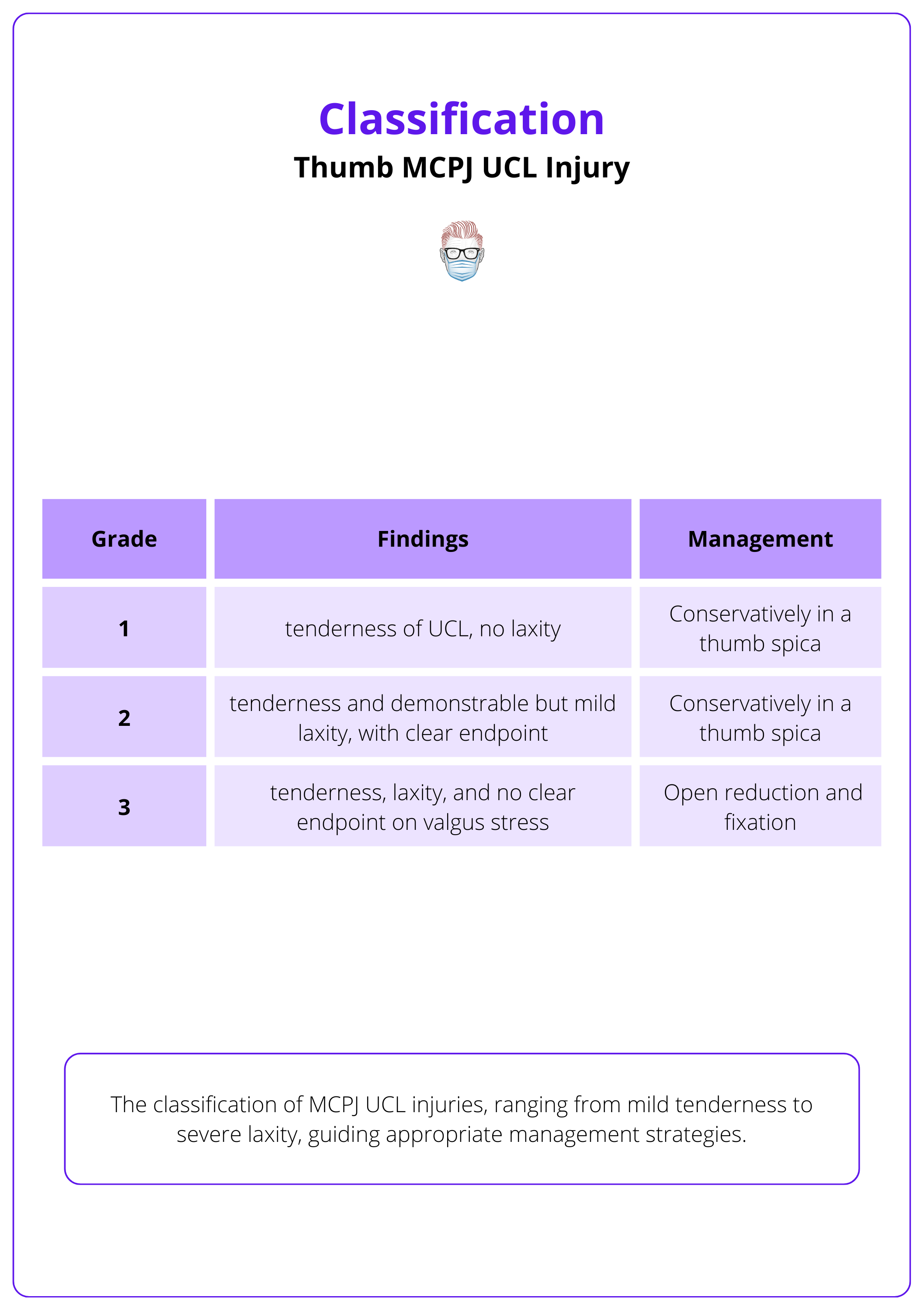
Thumb MCPJ UCL injuries can be classified by the degree of tenderness and laxity.
- Grade 1: tenderness of UCL, no laxity
- Grade 2: tenderness and demonstrable but mild laxity, with clear endpoint
- Grade 3: tenderness, laxity, and no clear endpoint on valgus stress
This classification guides the management of Grade 1 and 2 injuries. These can be managed conservatively in a thumb spica whilst open reduction and fixation is the mainstay of management for Grade 3 injuries.
This classification is explained in the table below.
In children, isolated rupture of the UCL without salter harris fracture is rare.
Investigations Thumb MCPJ UCL
Radiological investigations are commonly performed in suspected thumb UCL MPCJ injuries. These are usually X-rays, MRI, or Ultrasound.
Xray:
- AP/oblique and lateral X-rays should be taken to identify associated fractures.
- Stress X-rays may be obtained and dynamic fluoroscopy can be used to assess the range of motion and joint opening.
A typical fracture pattern associated with a thumb MCPJ UCL injury is illustrated in the image below.

Other Radiological Investigations:
- Ultrasound: high diagnostic accuracy for Stener Lesions (Qamhawi, 2021), more user dependent.
- MRI: demonstrate high diagnostic accuracy for Stener lesions (Qamhawi, 2021), more expensive, can result in false positives due the difficulty to distinguish thumb MPCJ UCL with fibrous scar tissue.
The image below shows the anatomy of the thumb injury in investigations.
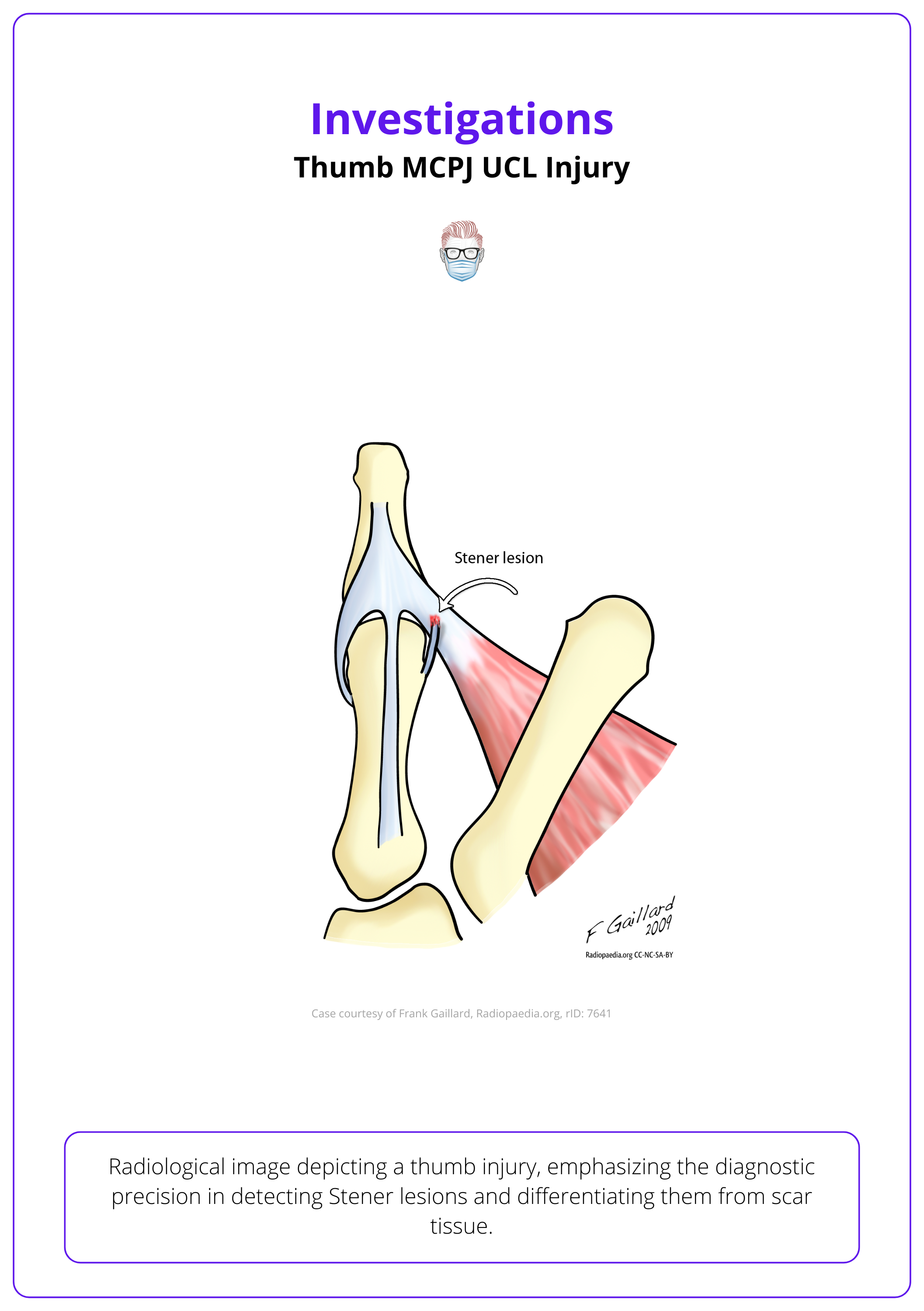
A Stener lesion occurs when the adductor aponeurosis is interposed between the UCL and MCP joint and prevents a completely avulsed UCL from approximating to its insertion. This requires surgical fixation to regain function.
Management of Thumb MCPJ UCL Injury
Conservative immobilisation is indication for partial thumb ligament tears. Chronic or complete tears require reinforcement (bone anchors, internal brace) or reconstruction (tendon graft).
Thumb MCPJ UCL injuries can be treated conservatively or surgically. This is influenced by the degree of laxity, presence of an endpoint and a Stener Lesion.
Conservative treatment
Conservative options includes 4 weeks of immobilisation, followed by 2 weeks in a lightweight splint. This is a common treatment protocol for acute partial tear injuries
- Initial Phase: 4 weeks of immobilization using a short arm thumb spica cast, leaving the interphalangeal joint free.
- Follow-up Phase: 2 weeks in a lightweight splint.
The indication for conservative treatment is a Grade 1 injury. Controversy remains regarding the most appropriate management of Grade 2 partial and complete tears with some surgeons opting for conservative management when a US and clinical examination do not detect a Stener lesion.
Surgical Repair Techniques
The surgical options available for the thumb MCPJ UCL injury include:
- Repair: primary repair in the acute setting
- Reinforce: Bone Anchors, Internal Brace/Suspension Tape
- Reconstruction: Chronic Injuries with Tendon graft (eg PL, FCR - Littler Technique)
Additional points to note on surgical interventions:
- Contraindication to surgical management is the presence of MCPJ osteoarthritis. This can occur in the chronic injury.
- Avulsed fragments greater than 2mm may be reduced and fixed using surgical screws. However, this is a matter of debate.
Early active movement facilitates good return of function and range of movement (Crowely, 2013).
Conclusion
1. Understanding Thumb MCPJ UCL Injury: You've gained a comprehensive understanding of the functional anatomy of the thumb, specifically focusing on the ulnar collateral ligament.
2. Identifying Injury Causes and Types: You've learned about the causes of thumb MCPJ UCL injuries, distinguishing between acute injuries often seen in sports (Skier’s thumb) and chronic conditions (Gamekeeper’s thumb), and how these conditions influence treatment decisions.
3. Diagnostic Strategies: You're now familiar with the diagnostic process for UCL injuries of the thumb, including clinical examination techniques to assess ligament damage and the presence of any associated avulsion fractures.
4. Thumb Injury Treatment Options: You now understand the management strategies for thumb MCPJ UCL injuries, ranging from conservative treatment for partial tears to surgical interventions for complete tears and certain avulsion fractures.
5. Surgical Techniques: You've reviewed various surgical techniques and their indications, which can help in planning the appropriate intervention based on the severity of the injury and the specific patient needs.
Further Reading
- Qamhawi Z, Shah K, Kiernan G, Furniss D, Teh J, Azzopardi C. Diagnostic accuracy of ultrasound and magnetic resonance imaging in detecting Stener lesions of the thumb: systematic review and meta-analysis. J Hand Surg Eur Vol. 2021 Nov;46(9):946-953. doi: 10.1177/1753193421993015. Epub 2021 Feb 17. PMID: 33596684.
- Avery DM 3rd, Caggiano NM, Matullo KS. Ulnar collateral ligament injuries of the thumb: a comprehensive review. Orthop Clin North Am. 2015 Apr;46(2):281-92. doi: 10.1016/j.ocl.2014.11.007. Epub 2014 Dec 30. PMID: 25771322.
- Sircar K, Dargel J, Scaal M, Eysel P, Müller LP, Wegmann K. Thumb metacarpophalangeal joint morphology and reconstruction of the ruptured ulnar collateral ligament. J Hand Surg Eur Vol. 2023 Sep;48(8):768-772. doi: 10.1177/17531934231164260. Epub 2023 Apr 2. PMID: 37005740.
- Crowley, Timothy P. MBChB, MRCS(Glasg); Stevenson, Susan MBChB, PhD, FRCS(Plast); Taghizadeh, Reika MBChB, FRCS(Plast); Addison, Patrick MBChB, MD, FRCS(Plast); Milner, Richard H. MD, FRCS(Plast). Early Active Mobilization Following UCL Repair With Mitek Bone Anchor. Techniques in Hand & Upper Extremity Surgery 17(3):p 124-127, September 2013. | DOI: 10.1097/BTH.0b013e318284dbd7
- Gluck JS, Balutis EC, Glickel SZ. Thumb ligament injuries. J Hand Surg Am. 2015 Apr;40(4):835-42. doi: 10.1016/j.jhsa.2014.11.009. PMID: 25813924.
