

Summary Card
Describing a Flexor Tendon Injury Repair
Tendon repairs are described by zone of injury, technique, material.
Zones of Flexor Tendon Repairs
Verdan's zones of repairs divide the volar hand into 5 zones.
Suture Technique for Flexor Tendons
Core sutures can range from 2-8 strands. This is a surgical decision.
The "Ideal" Flexor Tendon Repair
Strickland described the ideal repair focusing on core sutures, knot placement & several other factors.
Tendon Anatomy
Tendon anatomy involves collagen bundles and varied blood supply sources.
Tendon Healing
A tendon can heal through an extrinsic or intrinsic pathway through 3 phases: inflammation, proliferation and remodelling.
Describing a Flexor Tendon Injury Repair
Flexor tendon injury repairs are intricate procedures critical for restoring hand functionality after injury.
There are 3 common ways to describe flexor tendon injury repairs.
- Zone of injury: Zone 1-5 as described by Kleinert1 & Verdan2.
- Suture technique: eponymous name, core strands, configuration.
- Suture material: size, absorbable and non-absorbable.
This article will detail these 3 methods.
Zones of Flexor Tendon Repairs
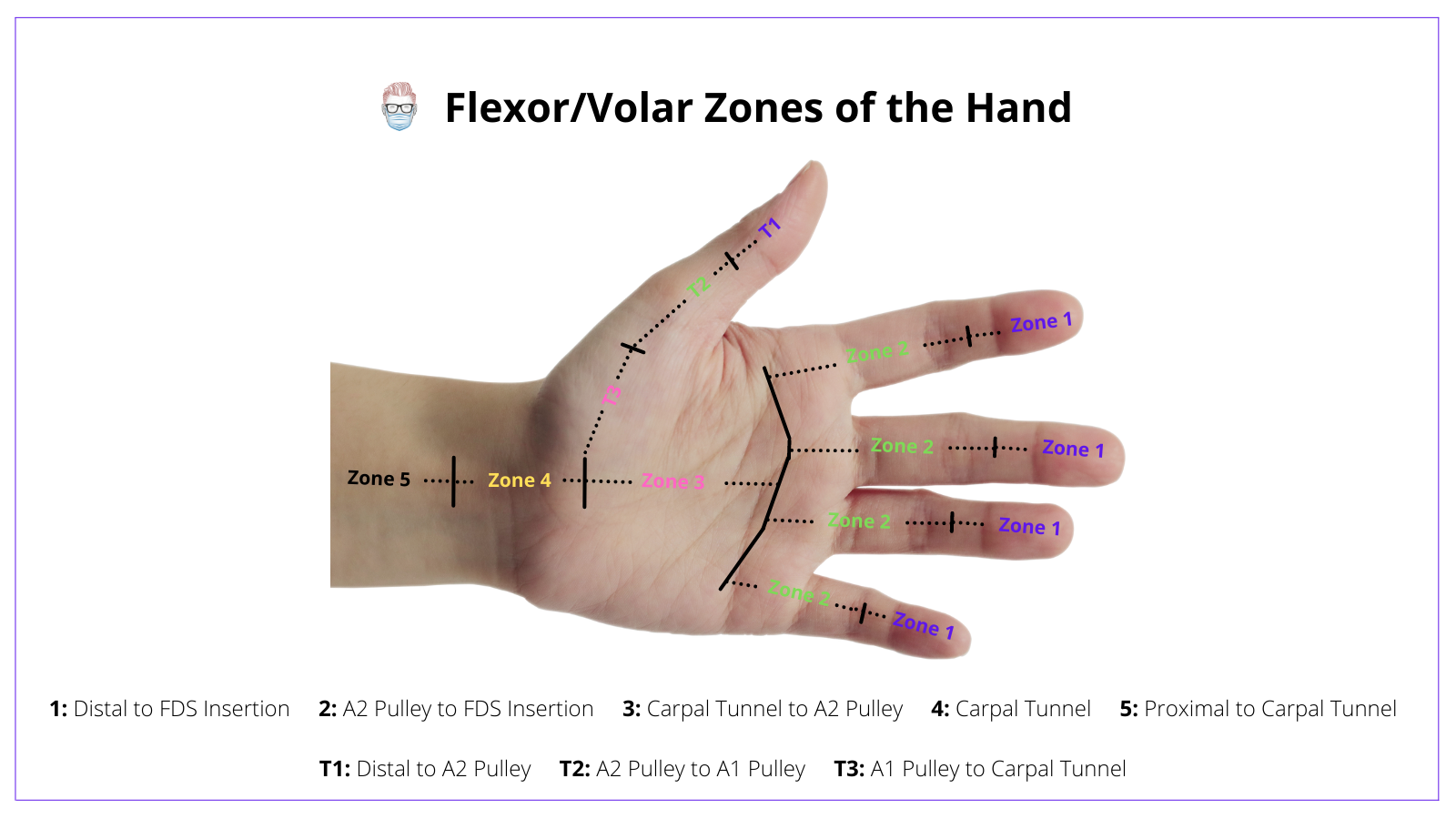
Zones of the Flexor Tendons were initially described by Kleinert and Verdan. There are 5 commonly described volar zones (zones 1-5).
Zones of Flexor Tendon injuries were popularised by Kleinert1 & Verdan2. They have an important role in providing:
- A universal language for flexor tendon injuries.
- Anatomical guide to pertinent structures.
- Predicting Rehabilitation Prognosis
Below is the visualization of the Flexor/Volar zones of the hand.
Check out the table below for the location of the Flexor/Volar zones of the hand and the clinical significance of each of them.
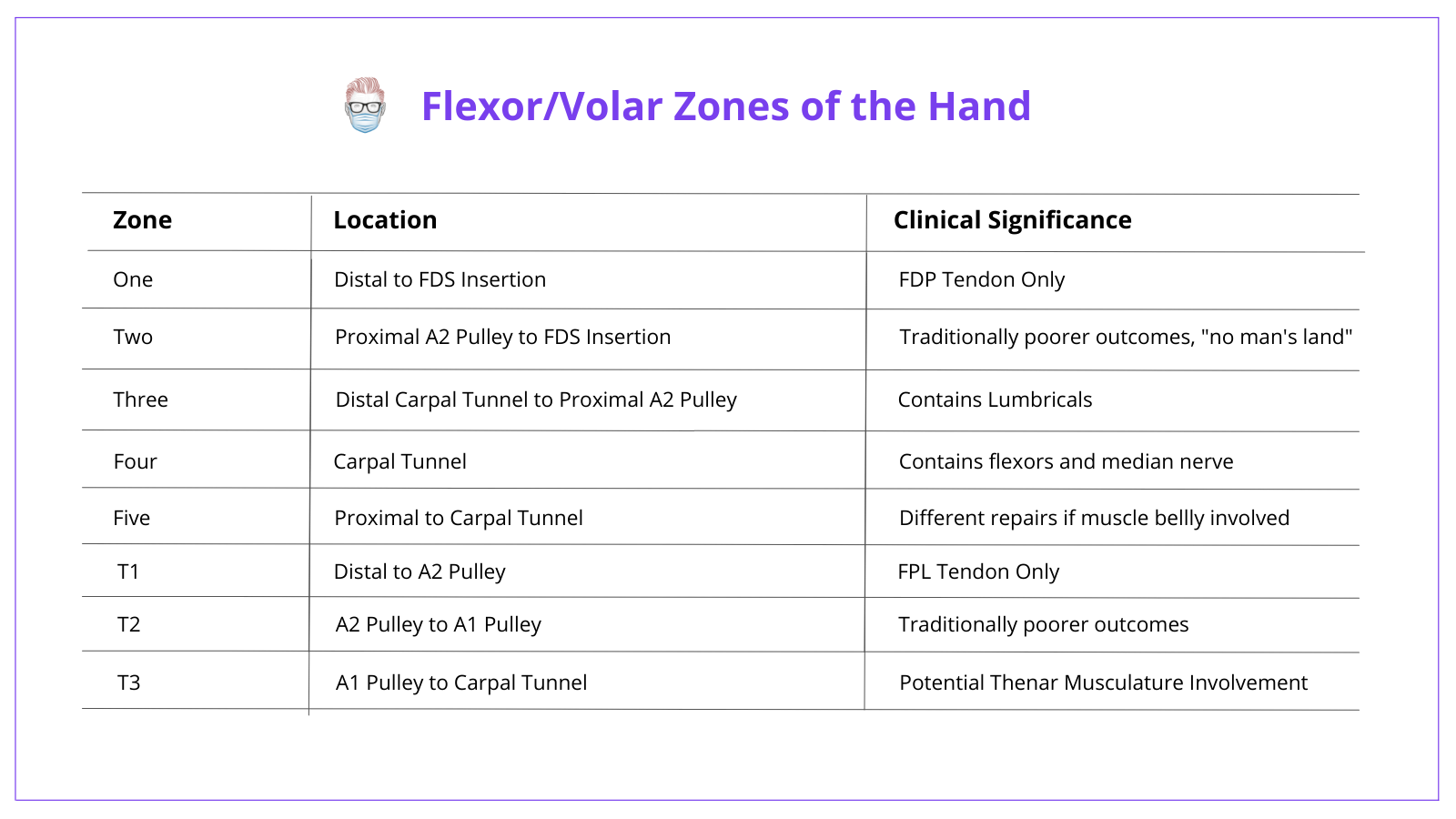
For more insights, check out this article on Zones of the Hand.
Suture Technique for Flexor Tendons
A flexor tendon repair can be described by its eponymous name, the number of core strands, configuration, knot location, and epitendinous suture.
There are a large number of variables deciding on your suture technique for flexor tendon injury repairs. It is further complicated by eponymous names (which are often incorrectly labeled).
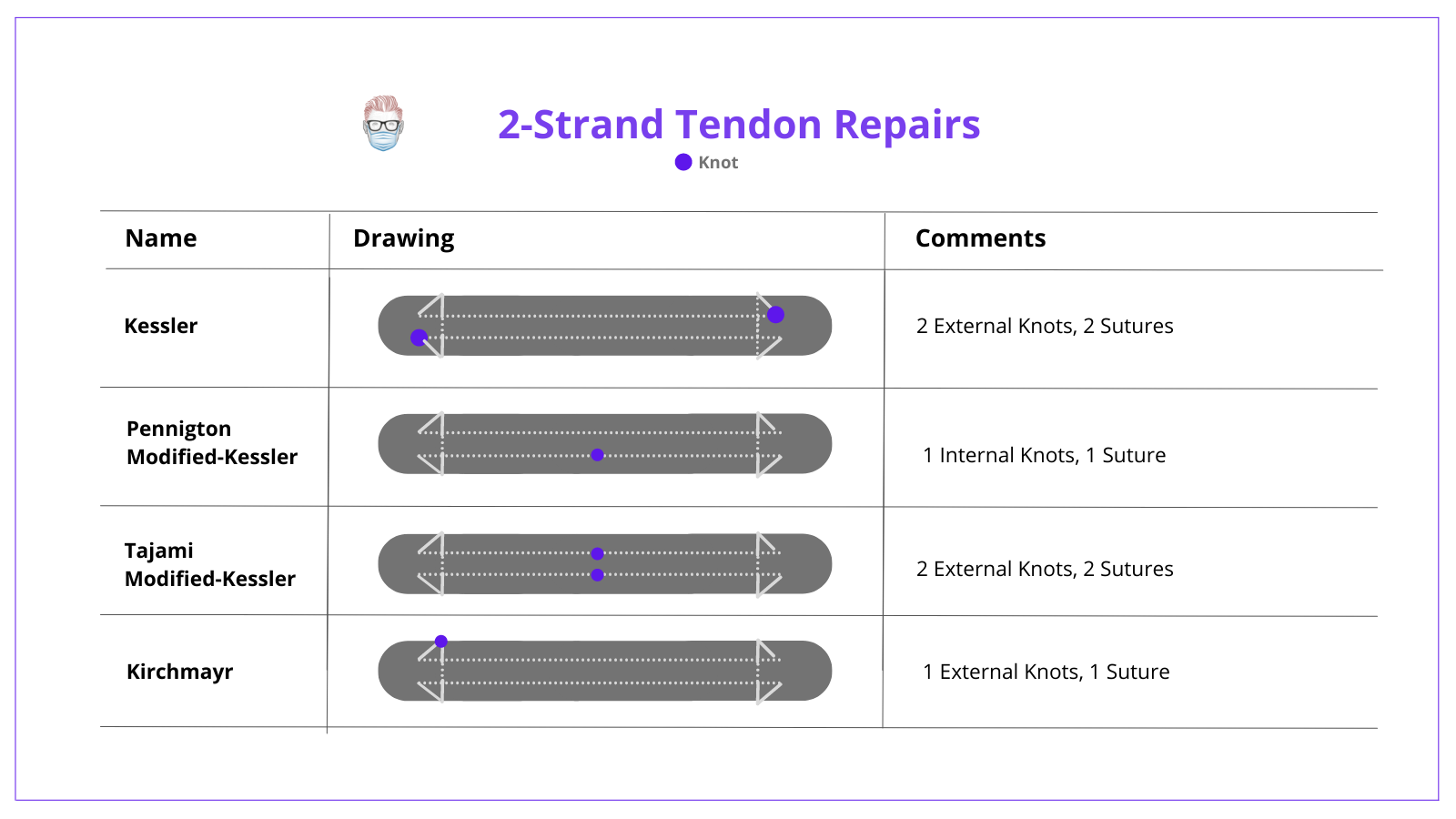
2-Strand Tendon Repairs
The table below details the different options for 2 strand tendon repairs. These are centered on the Kessler repair and its modifications.
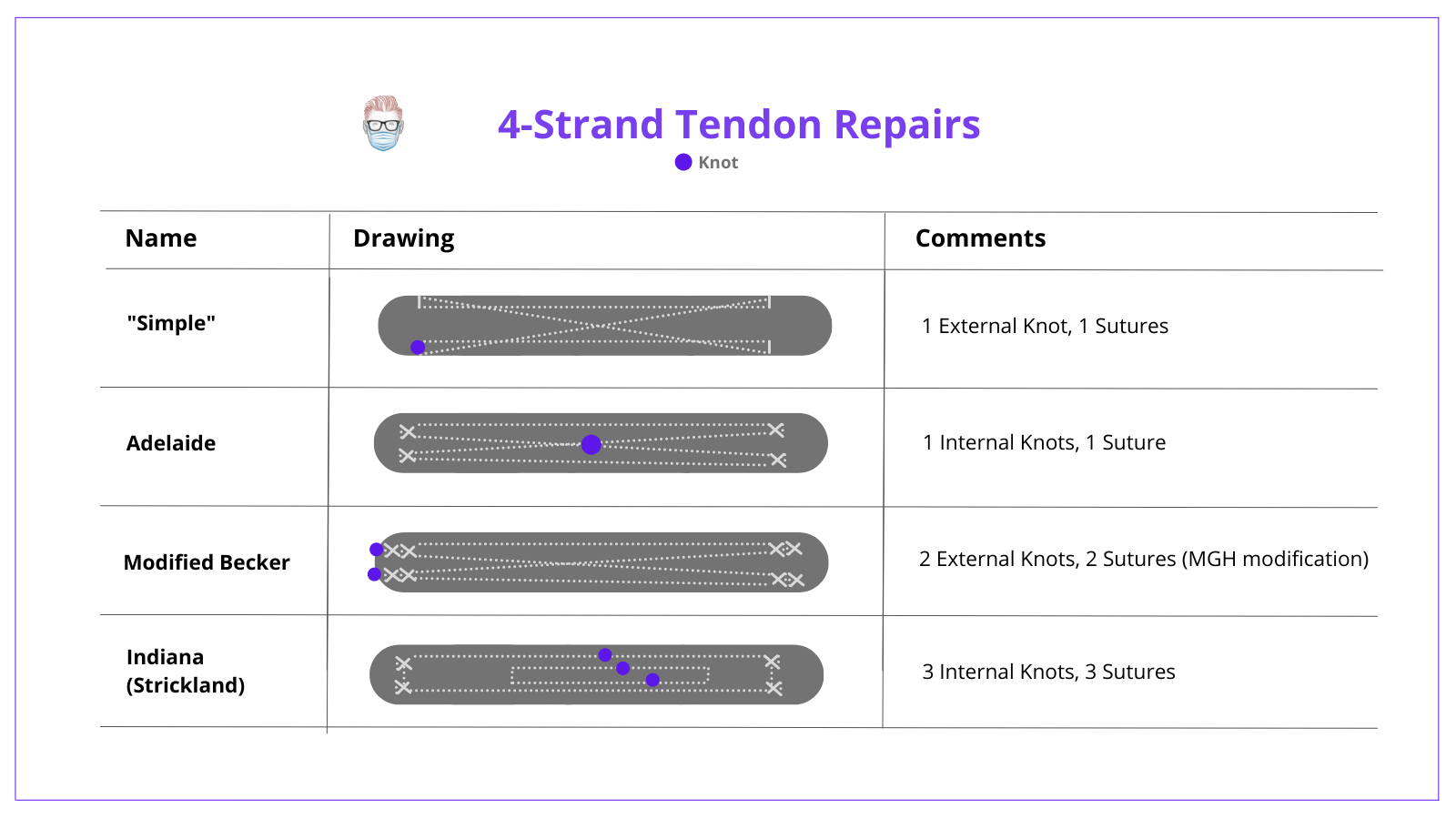
4-Strand Tendon Repair
It is generally accepted that 4-strand tendon repairs are the “minimum” number of core strands necessary for early motion exercises4. The table below summarizes the 4-strand tendon repairs.
As the technology and understanding of flexor tendon biology have increased, so too has the number of core strands. In literature and current clinical practice, 6-strand, and 8-strand flexor tendon repairs are used. These are listed below:
6-Strand
- Tsuge (Tang Modification)
- Savage (with Modifications)
- Lim-Tsai
8-Strand
- Knotless Barbed Suture
- Winters Gelberman
The "Ideal" Flexor Tendon Repair
Strickland described the ideal repair as having the following characteristics1:
- Easy suture placement
- Secured knots
- Smooth end-to-end tendon apposition
- Minimal to no gapping at the repair site
- Avoiding injury to tendon vasculature
- Having enough strength for early active postoperative motion
It is important to understand that there is "no gold standard" optimal repair algorithm.
Tendon Anatomy
Tendons are bundles of collagen wrapped in layers of adventitia with an array of blood supply sources.
Tendons are bundles of collagen arranged in a spiral fashion that contains fibroblasts, synovial cells and tenocytes. It can best be remembered by the "rules of 3":
1. There are 3 types of collagen:
- Collagen 1 (predominant)
- Collagen III
- Collagen IV
2. There are 3 main layers to the tendon:
- Endotendon: wraps the bundles of tendon
- Epitenon: the outer layer of synovial tendons
- Paratenon: a vascularised adventitial layer
3. There are 3 blood supply options:
- Vincular (not present in extensor tendons)
- Musculotendinous junction
- Bony insertions
Tendon Healing
A tendon can heal through an extrinsic or intrinsic pathway through 3 phases: inflammation, proliferation and remodelling.
Intrinsic and Extrinsic Pathways
These are two different mechanisms by which a tendon can heal.
- Extrinsic healing forms fibrous attachment between sheath & tendon that occurs in immobilised tendons
- Intrinsic healing is based on the early mobilisation of tendon injuries to allow blood flow and diffusion of nutrients from synovial fluid.
Phases of Wound Healing
There are 3 phases to wound healing: inflammation, proliferation and remodelling. There are the key components to each phase.
Inflammation
- Cells enter the wound
- Activation of growth factors
- Attraction of fibroblasts
Proliferation
- Fibroblasts secrete Type III collagen and GAGs.
- Disorganised arrangement of collagen (makes it weak)
Remodelling
- Begins ~3 weeks of injury repair
- Replacement of type III collagen with Type I collagen.
- Reorganization of collagen into a more organised structure (like wound healing)
Conclusion
1. Fundamentals of Flexor Tendon Repair: Gained a comprehensive overview of how flexor tendon injuries are repaired, emphasizing the importance of the injury's zone, suture techniques, and materials used.
2. Tendon Anatomy and Healing: Enhanced your understanding of the complex structure of tendons, their healing mechanisms, and the critical phases of tendon repair, from inflammation to remodeling.
3. Exploring Surgical Techniques: Delved into the specifics of various suture techniques, from 2-strand to 8-strand repairs, and the rationale behind choosing each based on the injury's specifics.
4. Importance of Epitendinous Repairs: Learned about the role of epitendinous repairs in improving the strength of the tendon repair and minimizing friction during the healing process.
5. Insights into Rehabilitation: Acquired knowledge on the rehabilitation process following flexor tendon repair, including the significance of early motion exercises and strategies to prevent adhesion formation, ensuring a successful recovery.
References & Contribution
Thank you to Amir Mahmoud Mohamed Labib Ghareib for helping create this article as part of the Authorship Program.
- Kleinert H, Kutz J, Ashbell T, et al: Primary repair of lacerated flexor tendons in “no man's land. J Bone Joint Surg Am 1967; 49: pp. 577
- Verdan CE: Half a century of flexor-tendon surgery: current status and changing philosophies. J Bone Joint Surg Am 1972; 54: pp. 472-491
- Strickland JW. Development of flexor tendon surgery: twenty-five years of progress. J Hand Surg Am. 2000;25(2):214e235.
- Chauhan, A., Palmer, B. A., & Merrell, G. A. (2014). Flexor Tendon Repairs: Techniques, Eponyms, and Evidence. The Journal of Hand Surgery, 39(9), 1846–1853.doi:10.1016/j.jhsa.2014.06.025
- Pruitt DL, Aoki M, Manske PR. Effect of suture knot location on tensile strength after flexor tendon repair. J Hand Surg Am. 1996;21(6):969e973.
- Labana N, Messer T, Lautenschlager E, Nagda S, Nagle D. A biomechanical analysis of the modified Tsuge suture technique for repair of flexor tendon lacerations. J Hand Surg Br. 2001;26(4): 297e300.
- Waitayawinyu T, Martineau PA, Luria S, Hanel DP, Trumble TE. Comparative biomechanic study of flexor tendon repair using FiberWire. J Hand Surg Am. 2008;33(5):701e708.
- Barrie KA, Wolfe SW, Shean C, Shenbagamurthi D, Slade JF, Panjabi MM. A biomechanical comparison of multistrand flexor tendon repairs using an in situ testing model. J Hand Surg Am. 2000;25(3):499e506.
- Joyce CW, Whately KE, Chan JC, Murphy M, O’Brien FJ, Carroll SM. Flexor tendon repair: a comparative study between a knotless barbed suture repair and a traditional four-strand mono-filament suture repair. J Hand Surg Eur Vol. 2014;39(1):40e45.
- Savage, R., & Tang, J. B. (2016). History and Nomenclature of Multistrand Repairs in Digital Flexor Tendons. The Journal of Hand Surgery, 41(2), 291–293.doi:10.1016/j.jhsa.2015.11.012
