
In this week's edition
- ✍️ Letter from P'Fella
Dogma has a long shelf life - 🖼️ Image of the Week
WALANT - Wide Awake Local Anaesthesia No Tourniquet - 🚑 Technique Tip
Microsurgery dogma: Do free flaps need prolonged bed rest? - 📖 What Does the Evidence Say?
Pressure sore recon: Does every sore need muscle underneath? - 🔥 Articles of the Week
Moist vs dry wound healing and suitable dressings. - 💕 Feedback
Suggest ideas & give feedback!
A Letter from P'Fella
Dogma Has a Long Shelf Life
That is usually how dogma works in real life. Not as something obviously wrong, but as something nobody feels the need to question anymore. A recent paper I read looked specifically at dogmas in plastic surgery and found challenged assumptions across flap surgery, hand surgery, wound healing, and craniofacial work, which tells you this is not a one-off problem in one tiny corner of the specialty.
The paper looked at commonly repeated perioperative practices in microsurgery and found that quite a few of the “standard” rules don’t hold up particularly well once you actually look at the evidence. Judicious vasopressor use appears safe. NSAIDs do not seem to raise hematoma or thrombosis risk. Routine therapeutic anticoagulation and dextran do not improve flap survival and add bleeding risk. Antibiotics beyond 24 hours do not seem to lower surgical site infection. Most vascular events happen in the first 48 to 72 hours, which makes some longer monitoring habits worth revisiting. Even older age, diabetes, and obesity on their own were not good reasons to rule patients out of microsurgical reconstruction.
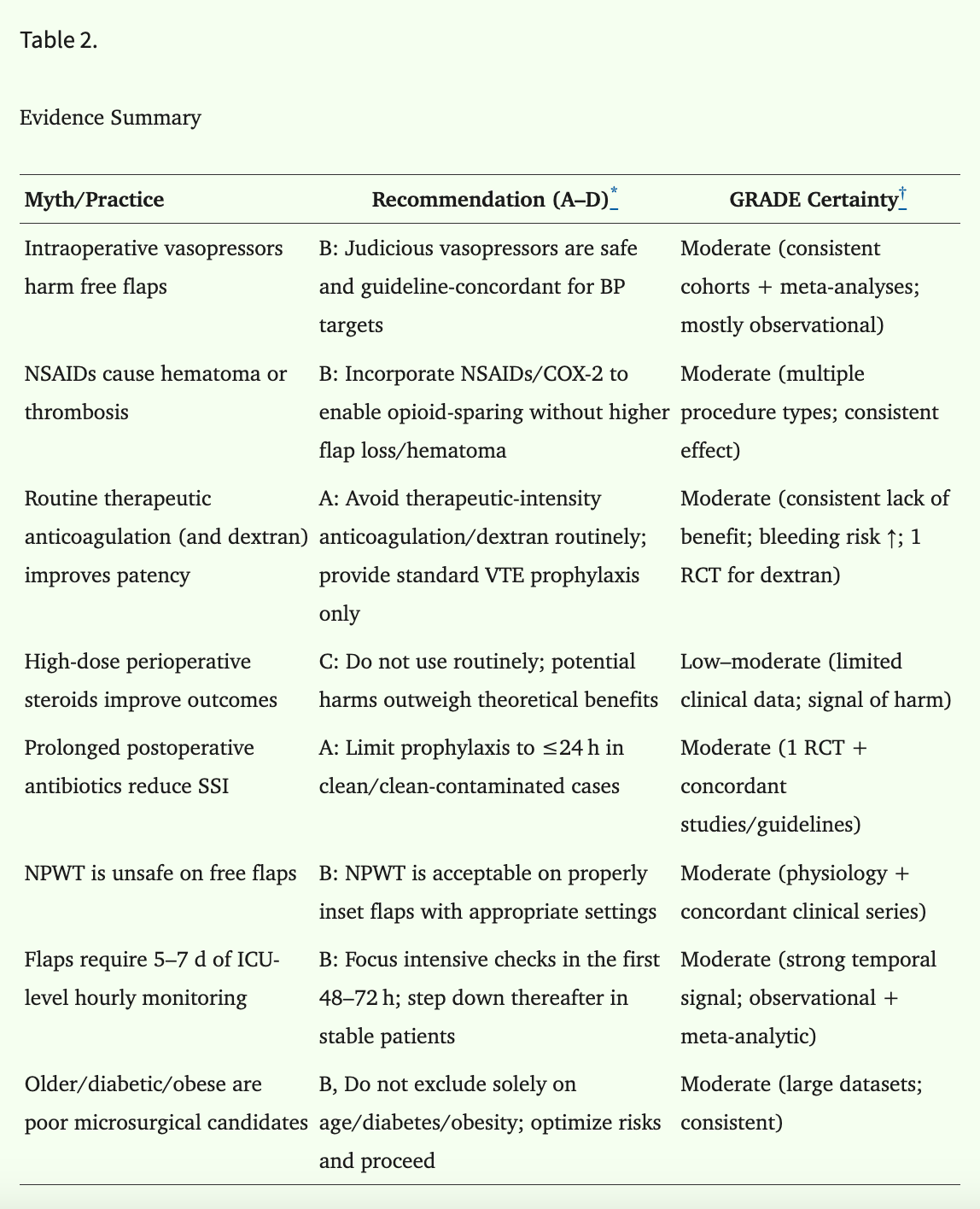
This table shows how much of practice can keep going long after the evidence has moved on.
What I find interesting is that this is not really a microsurgery problem. It is a surgery problem. Broader surgical work has shown that evidence can take years to change practice, and the barriers are usually very human ones: habit, selective memory, concern about complications, and the feeling that the old way is safer simply because it is familiar. In another recent study on surgical dogma, surgeons openly described reluctance to move away from long-standing practice, concerns about losing training opportunities, and the fact that personal experience often carries more weight than the paper in front of them.
That is why I like this topic. It isn’t about catching people out, and it isn’t about pretending every tradition is foolish. Some of the rules we were taught deserve to survive. Some probably don’t. The harder part is being perceptive enough to tell the difference. In plastic surgery, certainty travels very quickly, while evidence may take the longer route.
With love,
P’Fella ❤️
Image of the Week
WALANT - Wide Awake Local Anaesthesia No Tourniquet
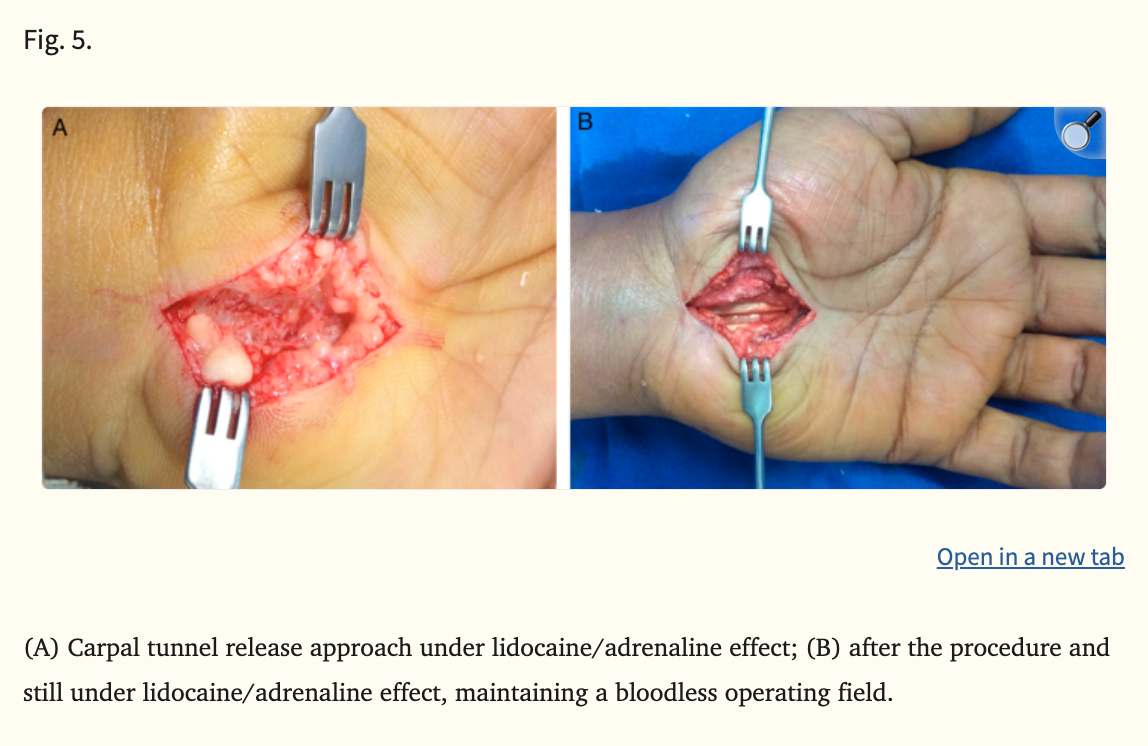
This week's image demonstrates a carpal tunnel release performed under WALANT (Wide Awake Local Anaesthesia No Tourniquet) using lidocaine with adrenaline.
The operative field remains remarkably bloodless despite the absence of a tourniquet, illustrating one of the most important paradigm shifts in modern hand surgery. For decades, surgeons were taught the dogma: “Never use adrenaline in the fingers or hand.”
Modern evidence has largely overturned this belief. In appropriately selected patients, epinephrine-containing local anaesthetic provides reliable vasoconstriction, improved visibility, reduced operative pain, and avoidance of general anaesthesia or tourniquet discomfort.
WALANT has since transformed hand surgery by enabling:
- Awake tendon assessment
- Outpatient procedures
- Reduced anaesthetic burden
- Greater operative efficiency
Technique Tip
Microsurgery Dogma: Do Free Flaps Really Need Prolonged Bed Rest?
Traditional lower-limb free flap care often involved strict bed rest, delayed dangling, no caffeine, and cautious mobilisation, largely from concern that dependency, vasospasm, or increased flow demand might compromise the anastomosis. Increasingly, this is being challenged: modern evidence suggests early, monitored dangling and mobilisation can be safe, with some studies showing reduced length of stay when protocols begin as early as POD1-5.
The key technical point is not “mobilise everyone early,” but replace ritual with monitored physiology. Assess flap colour, capillary refill, turgor, Doppler signal, and adjuncts such as tissue oximetry where available; stop dangling if perfusion parameters deteriorate. Similarly, blanket caffeine bans are increasingly difficult to justify, as recent reviews note limited evidence linking caffeine to flap loss.
What Does the Evidence Say?
Pressure Sore Reconstruction: “Every Sore Needs Muscle Underneath”
Clinical series support the same message. Retrospective pressure-sore cohorts show that recurrence and complication rates remain high regardless of flap type, and outcomes are heavily influenced by factors such as ulcer location, patient comorbidity, wound contamination, and the quality of off-loading and long-term care. Smaller comparative studies in sacral sores show that both fasciocutaneous and myocutaneous flaps can work, with no consistent universal winner.
Takeaway: Muscle is not mandatory beneath every pressure sore reconstruction; flap choice should be defect- and patient-specific, with enough tissue to fill dead space where needed, while preserving future reconstructive options whenever possible.
Sources: (Sameem, 2012); (Vathulya, 2022); (Chiu, 2017); (Oksman, 2018)
Articles of the Week
3 Interesting Articles with One-Sentence Summaries
Maintaining a moist wound environment (via appropriate dressings) accelerates healing by promoting keratinocyte migration, collagen synthesis, and autolytic debridement, while reducing pain and scarring compared to dry wound care.
Wounds treated in a moist or wet environment demonstrate faster re-epithelialisation, reduced inflammation, and improved scar quality compared to dry healing, while also enabling delivery of growth factors and cells to enhance regenerative outcomes.
Evidence consistently shows that wet-to-dry dressings delay healing, increase pain and infection risk, and are now considered substandard compared to modern moisture-retentive dressings that significantly improve wound outcomes and cost-effectiveness.
