
In this week's edition
- ✍️ Letter from P'Fella
We probably don’t teach delayed reconstruction properly enough - 🖼️ Image of the Week
Basal cell carcinoma: The facial “H-zone” - 🚑 Technique Tip
Excision of basal cell carcinoma - 📖 What Does the Evidence Say?
Defect-driven nasal reconstruction after BCC excision - 🔥 Articles of the Week
Facial BCC: Recurrence risk, Mohs vs standard excision, & non-Mohs eyelid BCC excision. - 💕 Feedback
Suggest ideas & give feedback!
A Letter from P'Fella
We Probably Don’t Teach Delayed Reconstruction Properly Enough
Most of the focus goes on margins, pathology, flap choice, and closure. The timing of reconstruction (when to close and when to wait) is usually picked up along the way rather than taught directly.
If you look at how patients experience this, it’s very different. The common questions are always about what happens next.
- Will it be closed on the same day?
- Why am I coming back?
- Who’s doing the reconstruction?
Because from their side, that gap between excision and reconstruction feels huge, even when it makes perfect clinical sense.
And I think that’s the bit we probably don’t teach properly enough. We spend a lot of time on margins, pathology, flap choices, grafts, and subunits. All important. But the decision of when to reconstruct is often treated like an afterthought, when in reality it can shape everything: the quality of the planning, the confidence of the surgeon, the availability of the right reconstructive input, and the conversation the patient has with the whole experience. Many clinical resources explicitly note that reconstruction after Mohs may be scheduled several days later, and recent conference discussion in dermatologic surgery has focused not just on how to close defects, but when to close them and when to refer.
That matters for trainees especially, because delayed reconstruction can look, on the surface, like hesitation. As if something has been left unfinished. But often it’s the opposite. Sometimes, delay is what allows you to do the reconstruction properly: once margins are certain, once the defect is fully understood, once the right surgeon is involved, once you’ve had time to choose the option that serves function and appearance rather than just ending the case quickly. That’s proper judgment.
So maybe this is one of the lessons that need more attention in skin cancer surgery: not every good reconstruction happens immediately, and not every immediate reconstruction is the best one. We probably need to talk about that more openly, teach it more deliberately, and explain it better to patients too. Delayed reconstruction isn’t a compromise. It’s part of doing the job properly.
With love,
P’Fella ❤️
Image of the Week
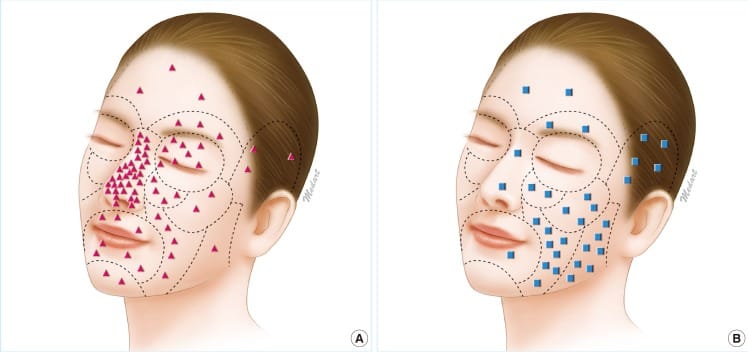
Basal Cell Carcinoma: The Facial “H-Zone”
This image demonstrates the distribution of basal cell carcinoma (BCC) across facial aesthetic units, highlighting the high-risk “H-zone” of the face.
The central face, including the nose, periorbital region, perinasal area, lips, and ears, represents a zone of increased tumour density, embryological fusion planes, and deeper tissue invasion. BCCs in this region are more likely to be aggressive, recurrent, and require tissue-sparing techniques such as Mohs surgery.
This has two key implications: Location determines both oncological risk and reconstructive strategy.
Technique Tip
Excision of Basal Cell Carcinoma
This video demonstrates simple excision of a BCC, the cornerstone of treatment for low-risk lesions. The key principle is complete tumour removal with appropriate margins, balancing oncological clearance with tissue preservation.
The technical takeaway is planning your excision before you cut: mark elliptical margins along relaxed skin tension lines, ensure adequate peripheral clearance, and perform layered closure to optimise healing. Early excision of small lesions is critical as delayed treatment leads to larger defects, more complex reconstruction, and worse cosmetic outcomes.
What Does the Evidence Say?
Defect-Driven Nasal Reconstruction After BCC Excision
When defects are larger, distal, or full-thickness, the forehead flap remains the most consistently supported workhorse option. In major Mohs-based nasal reconstruction series, it is repeatedly used for sizeable defects after BCC excision, while broader reviews of outer-nose BCC emphasise that convex nasal areas, especially the tip and ala, are reconstructively unforgiving and often need flap-based rather than simple secondary healing strategies.
The practical takeaway is that after oncologically sound BCC clearance, the best reconstruction is usually the one that restores contour and patency with the fewest stages necessary.
Sources: (Rohrich, 2004); (Moolenburgh, 2010); (Halani, 2021); (Boyd, 2000); (Wollina, 2014)
Articles of the Week
3 Interesting Articles with One-Sentence Summaries
After excision of eyelid basal cell carcinoma, recurrence risk is highest at the medial canthus and in sclerosing subtypes, and increases with each subsequent surgery, highlighting the importance of complete initial excision and consideration of adjuvant therapy in high-risk cases.
For facial basal cell carcinoma, Mohs micrographic surgery significantly reduces recurrence in recurrent tumours (≈2.4% vs 12.1%), but offers no significant advantage over standard excision for primary lesions, making case selection key.
Standard excision with ~4 mm margins can achieve very low recurrence rates (~4.3%) and even 0% in non-infiltrative BCC, but infiltrative histology and prior recurrence remain key predictors requiring long-term follow-up.
