

In this Article
Key Points
There are several described techniques for volar finger, hand and wrist incisions for different zones of the hand. The table below compares the two most commonly used in practice, Bruner and Mid-lateral.
| Bruner | Mid-Lateral | |
|---|---|---|
| Design | “Zig-Zag” | Straight-line |
| Location | Volar flexion crease | Dorsal to flexion crease |
| Flexor Exposure | Good | Good |
| Neurovascular Structures | Preserved | Division of dorsal branches |
| Scar | Volar surface with potential for sensitivity | Neutral position during flexion/extension |
Principles of a Hand Incision
The modern-day principles of hand incisions are largely founded on JM Bruner’s publications in 1951, 1966, 1967. Modifications do exist , as discussed below.
The “Perfect” Incision
The ideal hand incision should have the following1:
- Maximal exposure of the structures
- Minimal scarring and contracture (incisions cannot cross flexion creases)
- Minimal neurovascular and lymphatic disturbance
- Minimal impact on tendon gliding and joint motion
Types of Incisions
Several hand incisions have been described and the commonly used include:
- Zig-Zag Incision (Bruner)
- Mid-lateral incision (Bunnell)
- Antero-lateral Incision (Koch and Mason)
- Median Longitudinal Incision (McIndoe)
Anatomy of a Hand Incision
According to Bruner, the palmar creases of each finger joint have slight variation
- DIPJ: single crease
- PIPJ: double crease
- MCPJ: ring and middle finger has double crease, index and little has single crease.
According to Wood-Jones, between the flexion creases longitudinal lines are more prominent and represent the tension lines of Langer. These lines can be usual guide for limited incisions.
Bruner Incision
Design
A Bruner’s incision is a volar zig-zag incision between flexion creases designed with 3 key principles in mind:
- Reduce flexor contracture – straight-line incisions do not cross flexion creases.
- Ensure flap vascularity – flap angles are 90 degrees or greater
- Adequate access to structures – oblique incisions between flexion creases

In the 1950’s, “zig-zag” incisions became popularised for the surgical treatment of Dupuyteren’s disease. This was evolved into a volar approach to elective and non-elective hand conditions by Bruner in the 1950/1960s1,2.
Positive and Negatives
There is widespread acceptance for the utility of Bruner’s incisions. The following is a table discussing the pro’s and con’s of this surgical technique.
| Positives | Negatives |
|---|---|
| Good exposure to flexor tendons | Scar sensitivity |
| Direct access | Volar skin sensory disturbance |
| Preservation of neurovascular bundles | Contractures & adhesions still possible |
| Possible to extend into palm/wrist | |
Modifications
Midlateral Incision
Design
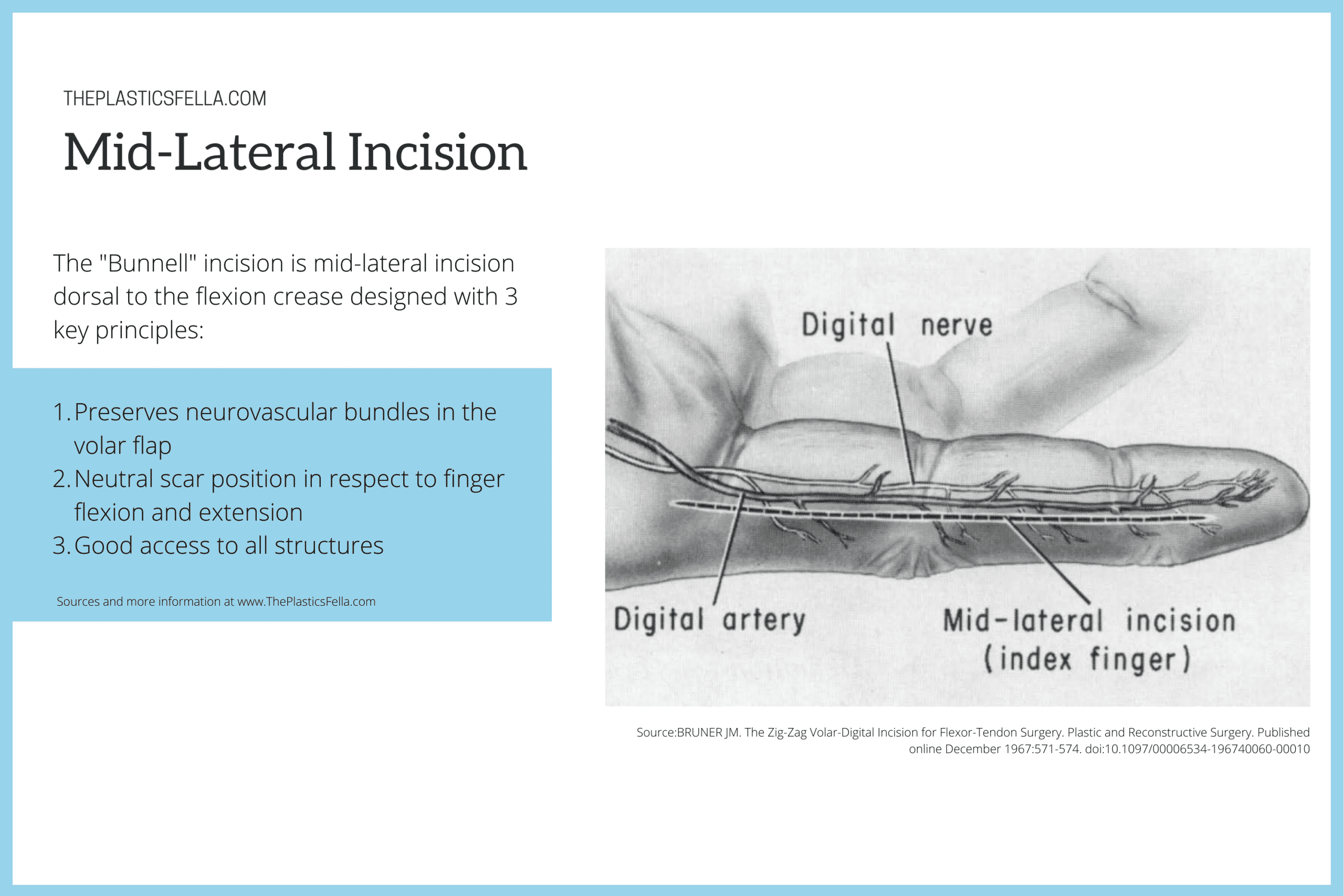
The “Bunnell” incision (1949) is mid-lateral incision dorsal to the flexion crease designed with 3 key principles:
- Preservation of neurovascular bundles in the volar flap
- Neutral scar position in respect to finger flexion and extension
- Good access to all structures
Positives and Negatives
The following is a table discussing the pro’s and con’s of this surgical technique.
| Positives | Negatives |
|---|---|
| Good exposure to flexor tendons | Indirect access to flexor tendons |
| Preservation of neurovascular bundles | Divides dorsal branches of Digital artery and nerve |
| Requires extension dissection, possible injury lateral structures (lateral bands, collateral and reticular ligaments) | |
| Can inhibit post-operative function if lateral structures damaged | |
Interestingly, the midlateral incision is preferred technique in Green’s Operative Hand Surgery for zone 1 and zone 2 flexor tendon repairs because it gives wide exposure and places intact skin and subcutaneous fat directly over the flexor tendon sheath.
Anterolateral Longitudinal Incision
This is a less commonly used technique.
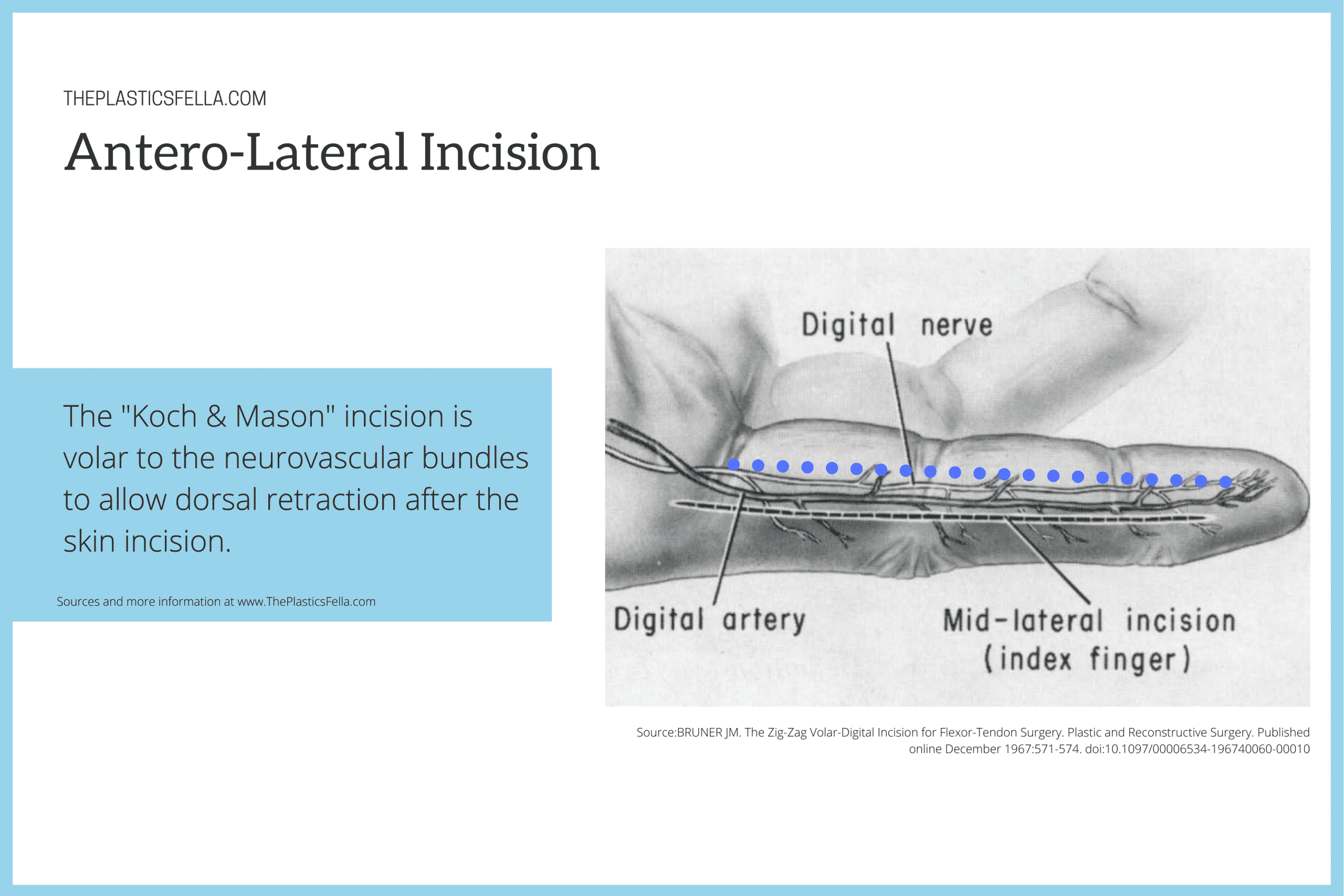
The antero-lateral longitudinal incision as used by Koch and Mason is designed on the principles of:
- Incision volar to the neurovascular bundle
- Dorsal retraction of neurovascular bundles after the skin is divide
References
- 1. Bruner JM. Incisions for plastic and reconstructive (non-septic) surgery of the hand. British Journal of Plastic Surgery. Published online 1951:48-55. doi:10.1016/s0007-1226(51)80006-7
- 2. BRUNER JM. The Zig-Zag Volar-Digital Incision for Flexor-Tendon Surgery. Plastic and Reconstructive Surgery. Published online December 1967:571-574. doi:10.1097/00006534-196740060-00010
- 3. Dancey A, Titley OG. A modification of the Bruner incision for the hand and review of the literature. Journal of Plastic, Reconstructive & Aesthetic Surgery. Published online September 2008:1130-1131. doi:10.1016/j.bjps.2008.05.004
- 4. Hall R, Vliegenthart D. A modified midlateral incision for volar approach to the digit. J Hand Surg Br. 1986;11(2):195-197. doi:10.1016/0266-7681(86)90258-5
