

Summary Card
Maxilla Reconstruction Anatomy
The maxilla has 1 body, 4 processes and 6 walls. It provides midfacial skeletal support and function for speech, swallowing and chewing.
Maxillectomy Indications
Benign or malignant tumours of the nose & paranasal sinuses. The commonest malignancy is squamous cell carcinoma & benign tumour is inverted papilloma.
Maxillary Classifications
Cordeiro classification describes 4 defects based on the number of walls, palate and orbital resection. It guides reconstruction options.
Maxillary Reconstruction Principles
The aim is to reconstruct the defect's volume, surface and components. Common options include RAFF, free rectus ± bone graft, and obturator insertion.
Maxillary Flap Reconstruction
Regional flaps, soft tissue, osteocutaneous flaps, and obturators, tailored to defect specifics and aimed at balancing aesthetics with function
Maxilla Reconstruction Algorithm
Large volume and surface area, consider rectus abdominis
Small surface area, consider radial artery forearm free flap
Bone defects consider bone grafts or vascularized bone flaps
Palate consider skin paddles or obturator.
Primary Contributor:
Waruguru Wanjau, Plastic Surgery Trainee, South Africa.
Maxilla Reconstruction Anatomy
The maxilla has 1 body, 4 processes and 6 walls. It provides midfacial skeletal support and function for speech, swallowing and chewing.
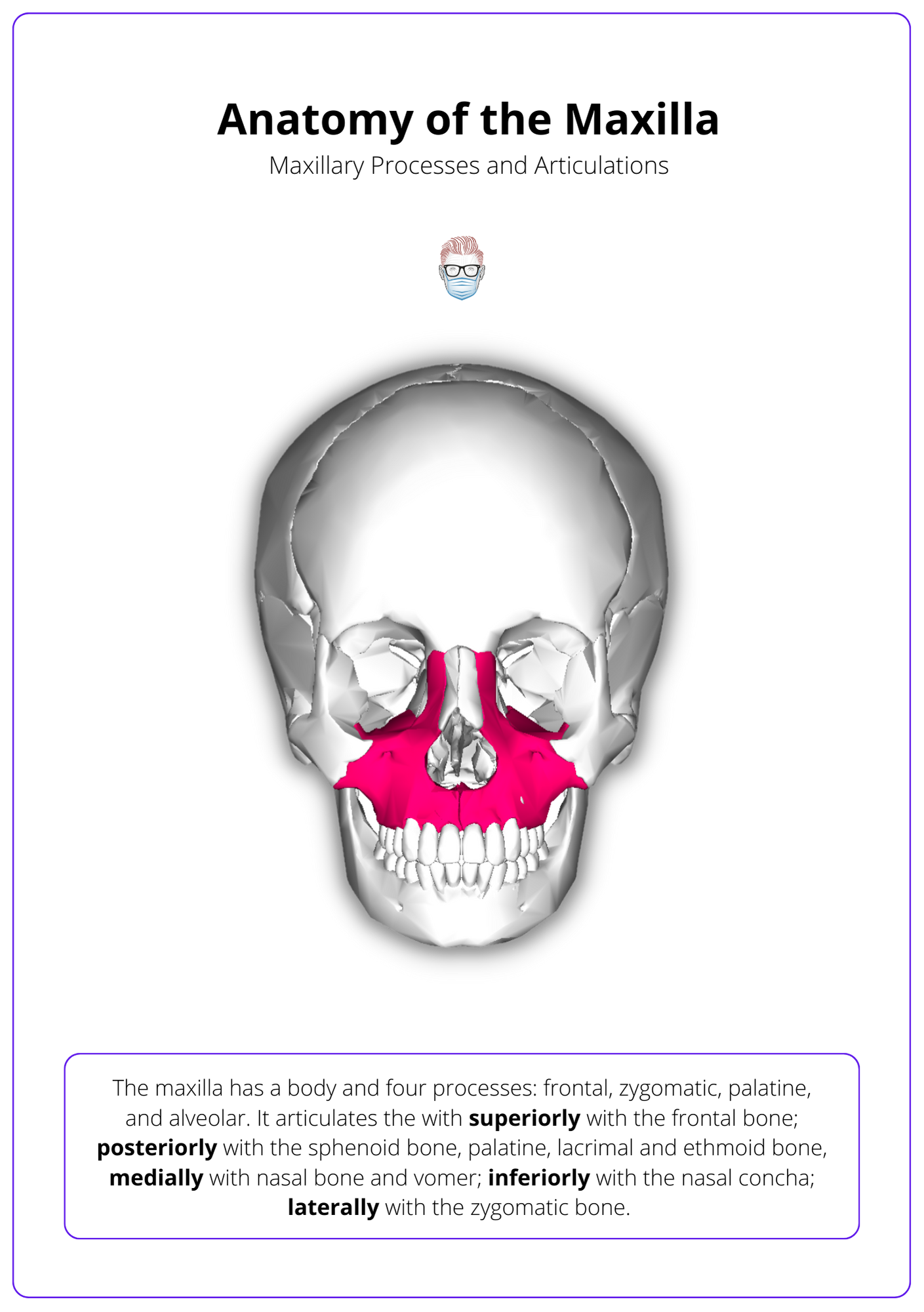
The maxilla consists of the a pyramidal body and its four processes: frontal, zygomatic, palatine, and alveolar.
It has several articulating surfaces, which include:
- Superiorly: frontal bone
- Posteriorly: sphenoid bone, palatine and lacrimal bones and ethmoid bone
- Medially with the nasal bone, vomer
- Inferior: nasal concha
- Laterally: with the zygomatic bone.
The maxilla contributes to the anterior margin and floor of the bony orbit, the nasal cavity and the infratemporal fossa. These cavities that need to be kept separate in the reconstruction of the maxilla.
It can be described as a hexahedrium (geometric structure with six walls) that creates a "maxillary antrum" within the central portion of the maxilla1.
- Roof: supports the ocular globe.
- Medial wall: a lateral wall of the nasal cavity and part of the lacrimal system
- Floor: anterior portion of the hard palate and alveolar ridge
- Buttresses: 2 horizontal and 3 vertical buttresses provide projection & height
- Other walls: formation of paranasal sinuses
The buttresses are key to the integrity of the maxilla and need to be considered during reconstruction of the maxilla. They are vertical and horziontal:
- Vertical: Nasomaxillary, Zygomatic, Pterygomaxillary
- Horizontal: Frontal, Orbital, Maxillary, Alveolar
The below image helps you better understand the anatomy of a Maxilla.

Maxillectomy Indications
Maxillary resections are usually for benign or malignant tumours of the nose and paranasal sinuses. The commonest malignancy is squamous cell carcinoma and benign tumour is inverted papilloma.
Maxilla resections can be indicated in malignant and benign tumours of the:
- Nose
- Paranasal sinuses of the nasal cavity
- Oral cavity tumour extending into the hard palate
- Treatment of fulminant invasive fungal sinusitis
Nasopharyngeal tumours are often treated with chemoradiotherapy and surgery has a more prominent role in recurrent disease.
The most common location of a tumour is the maxillary sinus, followed by the nasal cavity. The most common malignancy is squamous cell carcinoma. Other types of tumours include:
- Epithelial: adenocarcinoma, neuroblastoma, melanoma, adenoid cystic
- Sarcoma: osteosarcoma, chondrosarcoma. rhabdomyosarcoma
- "Benign": inverted papilloma, juvenile angiofibroma, osteoma, encephalocele (soft, blue, compressible neural tube defect).
A juvenile angiofibroma typically presents in males during their 2nd decade of life. This locally invasive benign tumour can cause life-threatening epistaxis. Treatment can be ligation or embolisation of the sphenopalatine artery, but not the anterior or posterior ethmoidal arteries (as these supply the retina!).
Maxillectomy Classifications
Cordeiro classification describes 4 defects based on the number of walls, palate and orbital resection. It guides reconstruction options.
A range of maxillary defect classification systems has been described, often within a broader category of complex midfacial defects2-4.
Cordeiro Classification
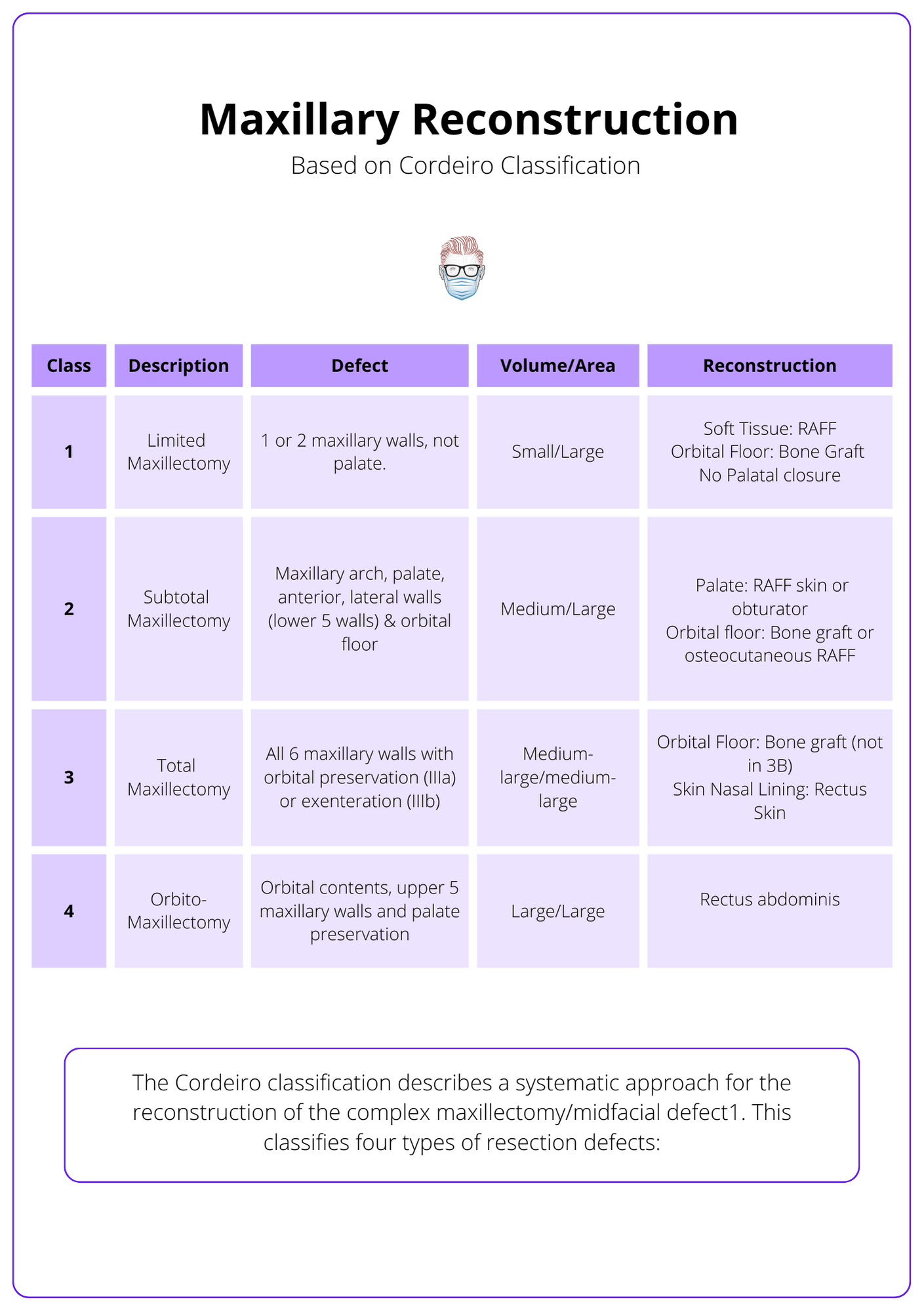
The Cordeiro classification describes a systematic approach for the reconstruction of the complex maxillectomy/midfacial defect1. It assesses the surface area to volume requirement, the need for orbital reconstruction and the need for palatal closure.
This classifies four types of resection defects:
- Type I Limited maxillectomy: one or two maxillary walls, excluding palate.
- Type II Subtotal maxillectomy: maxillary arch, palate, anterior & lateral walls (lower five walls), with preservation of the orbital floor.
- Type III Total maxillectomy: all six walls of the maxilla with orbital content preservation (IIIa) or exenteration (IIIb)
- Type IV Orbitomaxillectomy: orbital contents, upper five maxillary walls and preservation of the palate.
This classification system is used as a communication tool, for research and for guiding maxillary reconstruction algorithms.
Brown's Classifications
Brown et al. 4 published a modified classification system in 2000 to help guide treatment. It describes maxillary defects well both vertically and horizontally.
Vertical:
- Type I: maxillectomy not causing oronasal fistula
- Type II: not involving the orbit
- Type III: involving orbital adnexa with orbital retention
- Type IV: with orbital enucleation or exenteration
- Type V: orbitomaxillary defect
- Type VI: nasomaxillary defect
Horizontal classification:
- a—palatal defect only, not involving the dental alveolus
- b—less than or equal to 1/2 unilateral
- c—less than or equal to 1/2 bilateral or transverse anterior
- d—greater than 1/2 maxillectomy
Maxillary Reconstruction Principles
Maxillary reconstruction aims to reconstruct the defect's volume, surface and components. Common options include RAFF, free rectus ± bone graft, and obturator insertion.
The goal of maxillary reconstruction is to provide volume, soft tissue cover, support and preserve oral function (speech, swallowing and mastication)7. Reconstruction can be achieved either by using an obturator prosthesis or by surgical reconstruction.
The following key reconstructive principles should be adhered to:
- Reconstruct the type of defect (skin, soft tissue, palate, orbital floor, and bony structural deficits) and its volume and surface area.
- Obliterate dead space in the reconstructed maxillary walls with soft tissue (muscle/fat).
- Resurface intraoral cheek, palatal, nasal lining, or external resurfacing with skin paddles. Not all surfaces are necessarily relined. It is key to anatomically partition the oral and nasal environments
- Rebuild required support structures, such as the maxillary arch and orbital floor, with vascularized bone or bone grafts.
- Build walls between to recreate orbital and oropharyngeal cavities and separate the aerodigestive tract from intracranial space
Maxillary Flap Reconstruction
Maxillary reconstruction utilizes regional flaps, soft tissue, osteocutaneous flaps, and obturators, tailored to defect specifics and aimed at balancing aesthetics with function.
Generally speaking, surgical reconstructive options described for maxillectomy defects include:
- Regional soft tissue
- Free flaps with soft tissue alone
- Free flaps with bone
- Combinations of soft tissue flaps and alloplastic implants
Regional Soft Tissue Flaps
For regional maxilla reconstruction, selecting the appropriate flap type is critical based on defect characteristics.
- FAMM Flap: Ideal for small and relatively lateral defects.
- Buccal Pad of Fat: Suitable for small and relatively lateral defects.
- Reverse Submental Flap: Utilized for inferior maxillary defects.
- Temporalis Myofascial Flaps: Can lead to dehiscence in larger defects and may result in trismus. It can be transposed into the mouth, usually in older patients with contraindications for free flap surgery, not used for palatal reconstruction. It has a short arc of rotation.
Soft Tissue Free Flaps
Soft tissue free flaps are selected for cases where the orbital floor remains intact. In situations requiring additional bony support, augmentation with a free bone graft, titanium mesh or obturator prosthesis is an option. The benefit of free flaps includes
- Facilitate primary healing across extensive and intricate maxillofacial defects.
- Enhance support for maxillary buttresses and facial contours.
- Provide a robust base for subsequent dental implant placement.
Several soft tissue free flaps options do exist:
- Radial Forearm Flap: Features a long pedicle, simplifying vascular anastomosis in the neck area. Large surface area with small to medium volume defects. These can be fasciocutaneous or osteocutaneous.
- Rectus Abdominis: Benefits from large-caliber vessels and a low risk of atherosclerosis. May require flap revision, especially if excessive bulk persists post-radiation. Large volume with medium to large surface-area defects. It can provide skin to reline the maxillary sinus and repair the palatal defect. Risk of flap ptosis into the oral cavity.
- Anterolateral Thigh Flap: Offers the versatility of creating multiple skin paddles.
- Latissimus Dorsi: Similar to the Rectus Abdominis, there's a potential for flap ptosis into the oral cavity.
Osteocutaneous Flaps
Bone reconstruction is advisable for medium to large maxillectomy defects with a favorable oncologic outlook, especially when the restoration of oral function, midface aesthetics, and orbital structure are paramount. The integration of bone in maxillary reconstructions aims to:
- Reestablish the contour of the midface.
- Offer support to the orbital floor.
- Substitute the absent alveolar bone.
- Serve as an anchor for dental implants.
Many osteocutaneous flaps have been described:
- Fibula Osteocutaneous Flap: can be used to close the palatal defect to prevent nasal regurgitation, can also accept osseointegrated implants due to the good quality of bone stock associated with this flap. Adequate bone density for secure dental implant installation and extensive pedicle length. Limted by the fact it s insufficient soft tissue for maxillary cavity filling and inflexible for orbital floor support shaping.
- Coronoid Process of the Mandible (Temporalis Muscle): Challenges in mobilization. Limited soft tissue coverage.
- Superficial Temporal Artery (STA) and Vein-Based Calvarial Bone Flaps: Movement difficulties. Inadequate soft tissue coverage.
- Radial Forearm Osteocutaneous Flap: Extended pedicle. Broad skin paddle suitable for cheek or palatal coverage. Limited and thin bony portion.
- Deep Circumflex Iliac Artery-Based Iliac Crest Flap: Effective in restoring facial buttresses when placed vertically. Abundant cortical bone and potential muscle tissue. Short pedicle length. High donor site morbidity and excessive bulk. Limited soft-tissue flexibility relative to the bone.
- Scapula Flap: Capability to harvest multiple independent skin paddles, muscle, and bone from the lateral aspect of the scapula.
Additional Bone Flap Options:
- Rectus abdominis with ribs.
- Tensor fasciae latae (TFL) with iliac crest and internal oblique.
- Medial femoral condyle flap.
These considerations underscore the importance of flap selection tailored to specific reconstruction goals, balancing the need for bone support, soft tissue coverage, and the overall aesthetic and functional restoration of the maxilla
The Role of the Obturator
Prostheses can be used for obturation but are preferred for smaller defects. Prosthetic retention can be difficult or impossible in sizable defects, particularly when there are few teeth to stabilize the prosthesis. When considering the use of an obturator for maxilla reconstruction, it is crucial to evaluate both its benefits and limitations:
Advantages:
- Immediate dentition
- Able to monitor for recurrences
Disadvantages:
- Inadequate sealing leading to poor oro-nasal separation
- Instability of the prosthesis due to the lack of buttressing areas4
- Poor quality of life
- Poor quality speech
- Difficult to tolerate if radiation is considered5
Maxilla Reconstruction Algorithm
The Maxilla Reconstruction Algorithm highlights the importance of defect classification in determining tailored reconstructive strategies for maxillectomy defects.
Defect classification plays a pivotal role in guiding the selection of reconstructive strategies for maxillectomy, ranging from limited to extensive defects with varying needs for tissue replacement and structural support.
Cordeiro Classification
This table discusses maxillary reconstruction based on Cordeiro classification.
Type I Limited Maxillectomy:
- Small volume, large surface-area defect.
- Consider nonvascularized bone grafts, obturation & radial artery forearm flap.
Type II Subtotal Maxillectomy:
- Medium volume, large surface-area defects.
- Consider radial artery forearm flap (can reline palatal mucosal surface and nasal floor when folded over).
Type IIIA Total Maxillectomy with Sparing of Orbital Contents:
- Medium-large volume and medium-large surface-area defects.
- Require orbital floor reconstruction (bone grafts) and palatal reconstruction (the cutaneous aspect of a flap or obturator).
Type IIIB Total Maxillectomy with Orbital Exenteration:
- Large volume and large surface-area defects.
- Requires reconstruction of nasal lining (medial maxilla wall) & external defect with multiple skin islands.
- If the external skin is intact, a rectus-free flap with a skin island is used to close the palate, a second skin island to restore the lateral nasal wall, third skin island can be used to provide closure of the external skin deficit if necessary.
Type IV Defects: Orbitomaxillectomy
- Large volume and surface-area defects with an intact palate.
- Consider rectus abdominis flap to obliterate dead space and provide external skin resurfacing if needed.
Brown's Classification
In the context of maxillectomy defects and their reconstruction, Brown's classification provides a structured approach to match the type of defect with appropriate reconstructive options8:
- Class I: Maxillectomy Not Causing an Oronasal Fistula
- Reconstruction options include Obturation, Regional flaps, and Radial forearm flap.
- Class II: Defects Not Involving the Orbit
- Options for reconstruction are Obturation, Regional flaps, Radial forearm flap, Fibula flap, Deep Circumflex Iliac Artery (DCIA), and Scapula flap.
- Class III: Involving the Orbital Adnexae with Orbital Retention
- Reconstruction can be achieved with the Fibula flap, DCIA, Scapula flap, and Rectus abdominis flap.
- Class IV: With Orbital Enucleation or Exenteration
- Suitable reconstructive options include Rectus abdominis, Latissimus dorsi, DCIA, and Scapula flap.
- Class V: Orbitomaxillary Defect
- Reconstruction methods involve Temporalis flap, Radial forearm flap, Anterolateral Thigh (ALT) flap, Radial osteocutaneous forearm flap, and Thoracodorsal Artery Angular (TDAA) flap with scapula tip.
- Class VI: Nasomaxillary Defect
- The Radial osteocutaneous forearm flap and TDAA flap with scapula tip are recommended for reconstruction.
These classifications and corresponding reconstructive options provide a comprehensive guide for surgeons to tailor their approach based on the specific nature and extent of the maxillectomy defect.
Conclusion
1. Maxilla Anatomy and Importance: Understood the maxilla's anatomy, including its body, processes, and walls, emphasizing its role in midfacial skeletal support and functions such as speech, swallowing, and chewing.
2. Maxillectomy Indications: Gained knowledge about the reasons for undergoing maxillectomy, focusing on the treatment of benign and malignant tumors of the nose and paranasal sinuses, with specific mention of squamous cell carcinoma and inverted papilloma as the most common types.
3. Defect Classification Systems: Familiarized with the Cordeiro and Brown classifications for maxillary defects, which are essential for guiding the selection of appropriate reconstructive strategies post-maxillectomy.
4. Reconstruction Principles and Techniques: Gained insights into the principles of maxillary reconstruction for restoring the defect's volume, surface, and components. Learned about the use of different flaps and obturators, each with specific defect characteristics for the best aesthetic and functional outcomes.
5. Algorithm for Maxilla Reconstruction: Understood the structured approach of the reconstruction algorithm, helping in the selection of the most suitable reconstructive option based on the type and extent of the defect.
Further Reading
- Cordeiro PG, Santamaria E. A classification system and algorithm for reconstruction of maxillectomy and midfacial defects. Plast Reconstr Surg. 2000 Jun;105(7):2331-46; discussion 2347-8. doi: 10.1097/00006534-200006000-00004. PMID: 10845285.
- Spiro, R. H., Strong, E. W., and Shah, J. P. Maxillectomy and its classification. Head Neck 19: 309, 1997.
- Wells, M. D., and Luce, E. A. Reconstruction of midface defects after surgical resection of malignancies. Clin. Plast. Surg. 22: 79, 1995.
- Brown JS, Rogers SN, McNally DN, Boyle M. A modified classification for the maxillectomy defect. Head Neck. 2000 Jan;22(1):17-26. doi: 10.1002/(sici)1097-0347(200001)22:1<17::aid-hed4>3.0.co;2-2. PMID: 10585601.
- Cordeiro, P. G., and Santamaria, E. Primary reconstruc- tion of complex midfacial defects with combined lip- switch procedures and free flaps. Plast. Reconstr. Surg.
- Cordeiro, P. G., Santamaria, E., Kraus, D., et al. Reconstruction of total maxillectomy defects with preservation of the orbital contents. Plast. Reconstr. Surg. 102: 1874, 1998.
- Lenox ND, Kim DD. Maxillary reconstruction. Oral Maxillofac Surg Clin North Am. 2013 May;25(2):215-22. doi: 10.1016/j.coms.2013.01.004. PMID: 23642669.
- Brown, J.S. and Shaw, R.J., 2010. Reconstruction of the maxilla and midface: introducing a new classification. The lancet oncology, 11(10), pp.1001-1008.
