

Summary Card
Definition
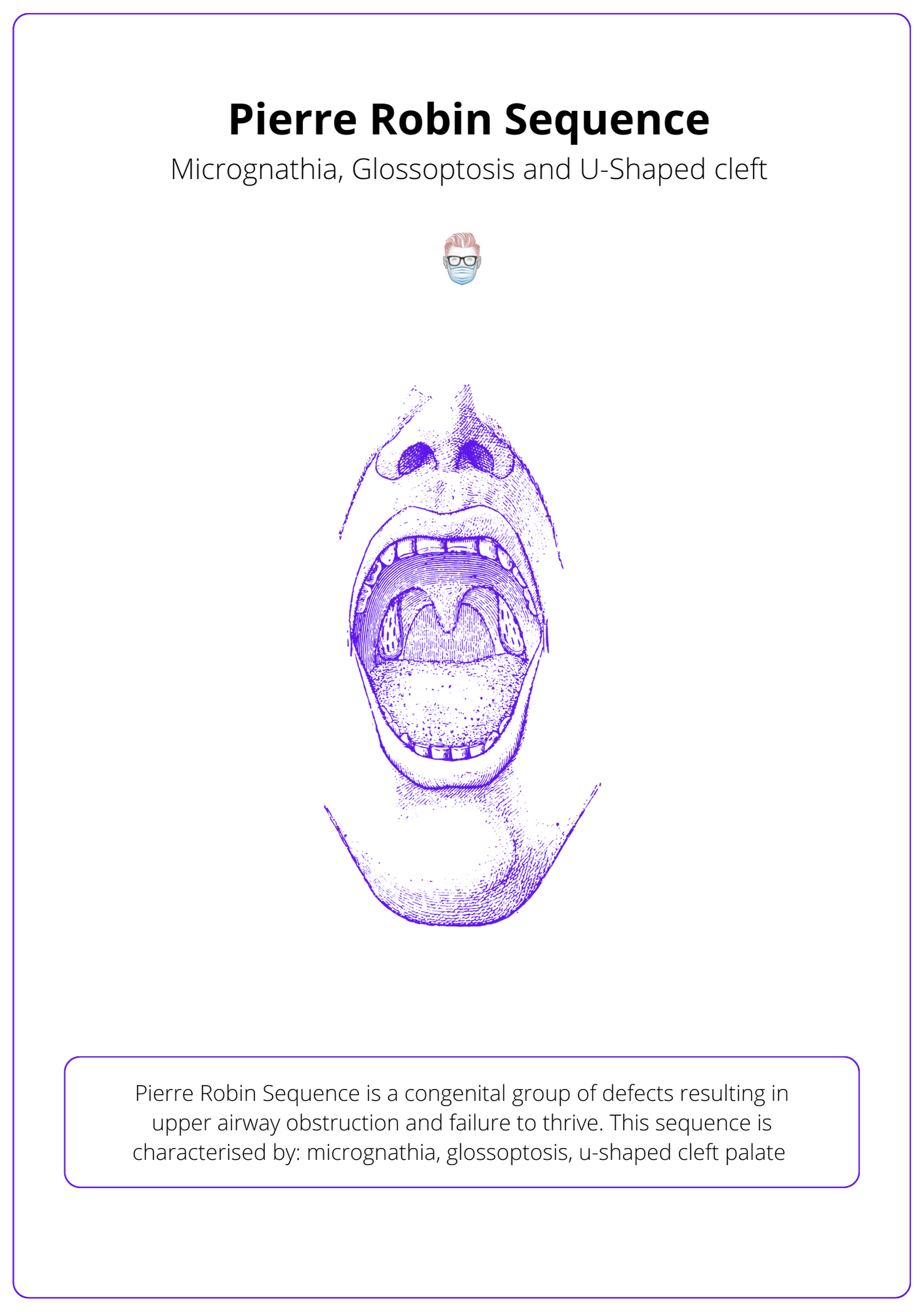
Micrognathia, Glossoptosis, and U-shaped Palate result in upper airway obstruction and failure to thrive.
Genetics
Rare and linked to Stickler, Nagar, and Treacher Collins Syndrome
Treatment
Acute management for airway and feeding. Long-term patients will often outgrow issues with airway and feeding.
Definition of Pierre Robin Sequence
Pierre Robin Sequence is a congenital condition characterized by a series of developmental defects leading to upper airway obstruction and failure to thrive, either as part of a syndrome or in isolation.
Pierre Robin Sequence is a congenital group of defects resulting in upper airway obstruction and failure to thrive. It can be syndromic or occur in isolation.
It is called a "sequence" because a single developmental defect results in a chain of secondary defects. More specifically:
- Defect 1: Micrognathia due to mandibular hypoplasia.
- Defect 2: Glossoptosis due to posterior displacement of the tongue.
- Defect 3: U-shaped cleft palate due to blocked closure of the palatal shelves.
A small jaw results in the tongue occupying a more significant proportion of the oropharynx and falling back to cause airway obstruction.
This sequence can be visualised in the illustration below.
Genetics of Pierre Robin Sequence
Pierre Robin Sequence has no specific identifiable genetic cause (yet). It is most commonly linked to Stickler Syndrome.
The incidence of the Pierre Robin sequence is ~1 in 8500-20,000 live births (Bush, 1983). To date, no specific human gene has been associated with the Pierre Robin sequence. There is a suggestion of a link to SOX9 and KCNJ2 mutations.
Pierre Robin Sequence is associated with (Marques, 1998):
- Stickler Syndrome – the risk of retinal detachment
- Nager Syndrome
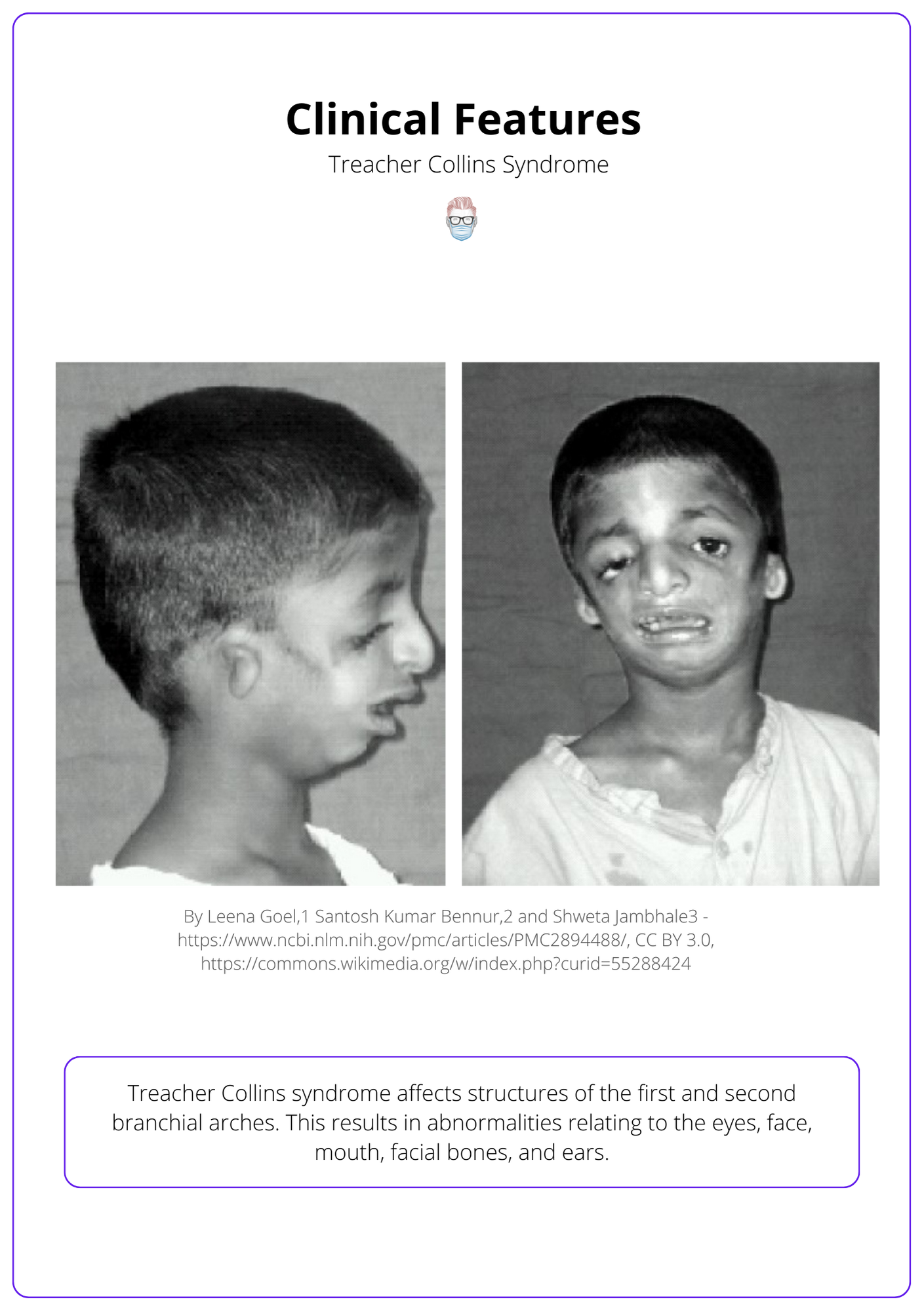
- Treacher Collins Syndrome
A patient with Treacher Collins Syndrome can be seen below.
Treatment of Pierre Robin Sequence
Acute management focuses on airway and feeding management. Considering longer term, patients can often outgrow their clinical issues.
Treatment is focused on the specific needs of each patient, but may include surgery to assist with breathing and feeding modifications to prevent choking. Generally, syndromic PRS patients are much more challenging to treat than those that occur in isolation.
Basic Airway Management
- Turn to the newborn prone to relieve the glossoptosis.
- A nasopharyngeal airway to bypass the obstruction caused by the tongue.
Advanced Airway Management
Advanced airway management options for the Pierre Robin Sequence include (Flores, 2014):
- Glossopexy: Tongue-lip adhesion for obstruction caused by glossoptosis (Kirschner, 2003).
- Tracheostomy
- Subperiosteal release of the floor of the mouth
- Distraction osteogenesis of the mandible (Cohen, 1999 & Tahiri, 2014) is an alternative to tracheostomy.
Prior to any surgical intervention, a nasoendoscopy is recommended. This is performed to rule out other anatomical sites or causes of airway obstruction
The mortality associated with these symptoms is between 1.7 and 11.3% (Smith, 2006).
Conclusion
1. Basica of Pierre Robin Sequence: Pierre Robin Sequence (PRS) is a congenital condition characterized by a series of developmental defects that result in upper airway obstruction and feeding challenges.
2. Recognition of Symptoms: You are aware of the physical manifestations of PRS, which primarily include micrognathia, glossoptosis, and a U-shaped cleft palate, leading to difficulties in breathing and feeding.
3. Associated Conditions: You understand that PRS can occur in isolation or as part of syndromes like Stickler, Treacher Collins, and Nager Syndromes.
4. Management: You've learned that initial management focuses on securing the airway and ensuring adequate nutrition, with long-term management often seeing improvement as the child grows.
5. Potential Surgeries: You are prepared to advise on possible future surgical interventions necessary if the child does not outgrow the breathing or feeding difficulties.
6. Treatment Challenges: You recognize the complexities of treating PRS, including the timing of any surgical interventions and the multidisciplinary approach needed for optimal care.
Further Reading
- Resnick CM. Precise osteotomies for mandibular distraction in infants with Robin sequence using virtual surgical planning. International Journal of Oral and Maxillofacial Surgery. January 2018:35-43. doi:10.1016/j.ijom.2017.07.020
- Robin P. A fall of the base of the tongue considered as a new cause of nasopharyngeal respiratory impairment: Pierre Robin sequence, a translation. 1923. Plast Reconstr Surg. 1994;93(6):1301-1303.
- Bush P, Williams A. Incidence of the Robin Anomalad (Pierre Robin syndrome). Br J Plast Surg. 1983;36(4):434-437. doi:10.1016/0007-1226(83)90123-6
- Marques I, Barbieri M, Bettiol H. Etiopathogenesis of isolated Robin sequence. Cleft Palate Craniofac J. 1998;35(6):517-525. doi:10.1597/1545-1569_1998_035_0517_eoirs_2.3.co_2
- Poswillo D. The aetiology and pathogenesis of craniofacial deformity. Development. 1988;103 Suppl:207-212.
- Sher A. Mechanisms of airway obstruction in Robin sequence: implications for treatment. Cleft Palate Craniofac J. 1992;29(3):224-231. doi:10.1597/1545-1569_1992_029_0224_moaoir_2.3.co_2
- Cohen M. Robin sequences and complexes: causal heterogeneity and pathogenetic/phenotypic variability. Am J Med Genet. 1999;84(4):311-315.
- Flores R, Tholpady S, Sati S, et al. The surgical correction of Pierre Robin sequence: mandibular distraction osteogenesis versus tongue-lip adhesion. Plast Reconstr Surg. 2014;133(6):1433-1439. doi:10.1097/PRS.0000000000000225
- Kirschner R, Low D, Randall P, et al. Surgical airway management in Pierre Robin sequence: is there a role for tongue-lip adhesion? Cleft Palate Craniofac J. 2003;40(1):13-18. doi:10.1597/1545-1569_2003_040_0013_samipr_2.0.co_2
- Tahiri Y, Viezel-Mathieu A, Aldekhayel S, Lee J, Gilardino M. The effectiveness of mandibular distraction in improving airway obstruction in the pediatric population. Plast Reconstr Surg. 2014;133(3):352e-359e. doi:10.1097/01.prs.0000438049.29258.a8
- Smith M, Senders C. Prognosis of airway obstruction and feeding difficulty in the Robin sequence. Int J Pediatr Otorhinolaryngol. 2006;70(2):319-324. doi:10.1016/j.ijporl.2005.07.003
