
In this week's edition
- ✍️ Letter from P'Fella
The ideas that change how we work - 🎧 How I Operate
Episode 2 releasing tomorrow! - 🖼️ Image of the Week
Latissimus Dorsi: Type V in action - 🚑 Technique Tip
Gracilis myocutaneous free flap harvest - 📖 What Does the Evidence Say?
Reverse-flow flaps: Why the vein matters most - 🔥 Articles of the Week
Perforator flaps & the lower trapezius musculocutaneous flap. - 💕 Feedback
Suggest ideas & give feedback!
A Letter from P'Fella
The Ideas That Change How We Work
A few do something else entirely. They stop being just papers and become part of the way a specialty thinks.
That’s what happened with Mathes and Nahai. At some point, it just became the language people use when they talk about muscle flaps. Type I. Type II. Type V. Dominant pedicle. Secondary segmental supply. Once an idea starts doing that, it’s no longer just living on the page.
What’s interesting is that this usually doesn’t happen because the underlying subject is simple. Muscle vascular anatomy isn’t simple. Flap behaviour isn’t simple. What lasts is when someone manages to take something complicated and present it in a way that's simple enough for most to grasp. A lot of clever ideas get dismissed because a majority can't carry them. They’re too messy, too buried in detail, too badly explained, or too difficult to teach. The ideas that survive are the ones that break down the complexity, instead of making it even more complex.
The Mathes and Nahai publication gave surgeons a framework they could actually use. You could teach it, test it against real anatomy, and apply it in theatre. You could explain why the latissimus behaves one way and the gracilis another. You could predict what changes when the pedicle changes. The contribution wasn't simply discovering something, it was figuring out the way to break it down in a way for everyone to understand
When it comes to lasting concepts in surgery, it’s not only about whether the idea was right, although that obviously is the key thing. An idea needs to be communicated clearly enough, taught well enough, and built simply enough that those who come after you could pick it up and actually use it. Otherwise, good ideas might stay trapped with the people who first discovered them.
We’re releasing my conversation with Professor Foad Nahai tomorrow, and it’s really about where one of those rare ideas came from. Not just the anatomy, but the thinking, the presentation, and why it managed to last. If you haven’t already subscribed, keep an eye out for it tomorrow!
P’Fella ❤️
How I Operate
Episode 2 Releasing Tomorrow!
More than 40 years after its publication, the classification remains one of the core frameworks in plastic surgery training. In this conversation, Professor Nahai reflects on the anatomy lab work, clinical problems, and collaboration with Dr Stephen Mathes that led to a system still used to understand muscle flap vascular anatomy today.
Stay tuned for Monday’s release!
How I Operate - Episode 2
Image of the Week
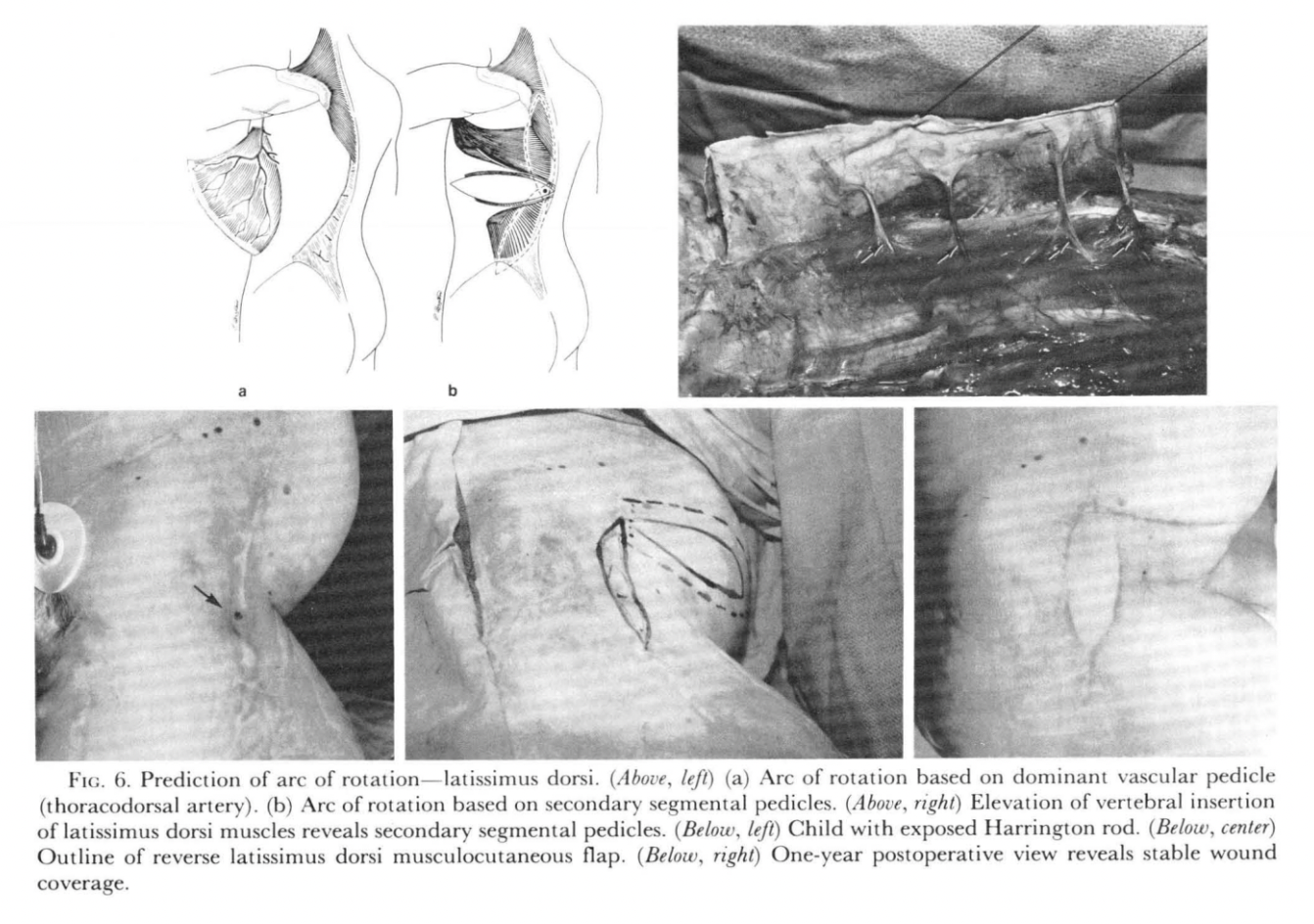
Latissimus Dorsi: Type V in Action
This week's image is from the original Mathes and Nahai publication, illustrating the principle that blood supply determines what a flap can do. The latissimus dorsi is a Type V muscle with one dominant pedicle (thoracodorsal) and additional segmental perforators.
The diagrams highlight the key idea: change the pedicle, and you change the arc of rotation. This is what makes the reverse latissimus possible. The operative image reinforces that preserving segmental vessels creates options when the main pedicle isn’t usable.
This is the core of the classification: predicting how far a flap can safely reach, and under what conditions.
Technique Tip
Gracilis Myocutaneous Free Flap Harvest
The gracilis is a classic Mathes & Nahai Type II muscle flap, supplied by a single dominant vascular pedicle with additional minor pedicles. Its reliable anatomy, long pedicle, and minimal donor-site morbidity make it a versatile option for free tissue transfer in head and neck, perineal, and extremity reconstruction.
This operative video demonstrates the key steps of gracilis flap harvest, including muscle identification, pedicle dissection, preservation of the skin paddle, and flap elevation.
What Does the Evidence Say?
Reverse-Flow Flaps: Why the Vein Matters Most
Reverse-flow flaps opened up reconstructive options without microsurgical transfer or sacrifice of a major axial vessel. Studies have shown that the reverse-flow posterior tibial artery island flap can be a reliable option for foot defects, supporting the idea that reverse perfusion can be dependable in carefully selected cases. The distally based superficial sural flap then became a major workhorse for the distal third of the leg, ankle, and heel, precisely because it exploits this same reverse-flow principle through peroneal perforators and the sural vascular axis.
While reverse-flow flaps do not “break” vascular rules, they depend on understanding them more deeply, especially the balance between retrograde inflow and precarious venous return.
(Torii, 1987); (del Pinal, 1993); (Liu, 1990); (Hasegawa, 1994); (Almeida, 2002)
Articles of the Week
3 Interesting Articles with One-Sentence Summaries
Perforator flaps achieve reliable reconstruction while minimising donor site morbidity by preserving muscle, but require precise anatomical understanding and careful perforator selection to maximise their versatility and outcomes.
All perforator flaps can be reduced to a simple principle of vascular anatomy, with reliability determined by whether the perforator reaches the skin directly or indirectly, guiding flap design and predicting outcomes.
The lower trapezius musculocutaneous flap offers a long, consistent pedicle via the dorsal scapular artery with low donor morbidity, but requires precise anatomical understanding to safely extend its arc of rotation or use it as a free flap.
