
In this week's edition
- ✍️ Letter from P'Fella
Working on the next department - 🖼️ Image of the Week
ICG lymphography patterns in early lymphatic dysfunction - 🚑 Technique Tip
Guide to Lymphaticovenous Anastomosis (LVA) - 🎓 Building in Public
How I Operate: Releasing soon! - 📖 What Does the Evidence Say?
Reverse lymphatic mapping in VLNT - 🔥 Articles of the Week
ICG velocity, lymphedema pathophysiology, & dermal backflow patterns - 💕 Feedback
Suggest ideas & give feedback!
A Letter from P'Fella
Working on the Next Department
The Cosmetics team has been a really eye-opening pilot for us because it’s shown us how building a department works in real life. Not just on a planning doc, but in the day-to-day process of taking an article and trying to make it educational, clear, and useful for trainees. That’s probably been the most helpful part so far. It’s shown us where the process already works, where it needs improvement, and what good collaboration actually looks like when everyone is working with the same goal in mind.
A lot of that has come down to feedback. The On-Call Team has been keen from the start. Thoughtful, sharp, and willing to get past the surface. Good article review is not just about spotting what’s technically wrong. It’s about knowing how to make the teaching better. Benedetta Agnelli, our clinical lead, has played a big part in helping us put a proper system around that, so the feedback is honest, guided, and actually useful rather than generic and vague.
At the same time, the Core Team has been working closely with the On-Call Team on how to improve the feedback itself, so the review process gets stronger and more consistent each round. That’s what gives us the best chance at publishing articles that don’t just say the right things, but teach them well.
We’ve also been spending more time on the visual side of these articles, including clinical images, diagrams, guides, and other teaching aids. Those are often the bits that make something click more quickly. That part is still evolving, but it’s already changing how we think about these articles. Not just what they should contain, but what they should actually do for the person reading them.
The team is getting along well, the process is sharper than it was when we first launched, and there’s a lot more confidence in how to do this properly. So now, we’re getting ready to do the same with the Lymphovascular Department. We’ve reattached the form below for anyone who missed it the first time and wants to be part of the next department. Let’s build this together 👇
P’Fella ❤️
Image of the Week
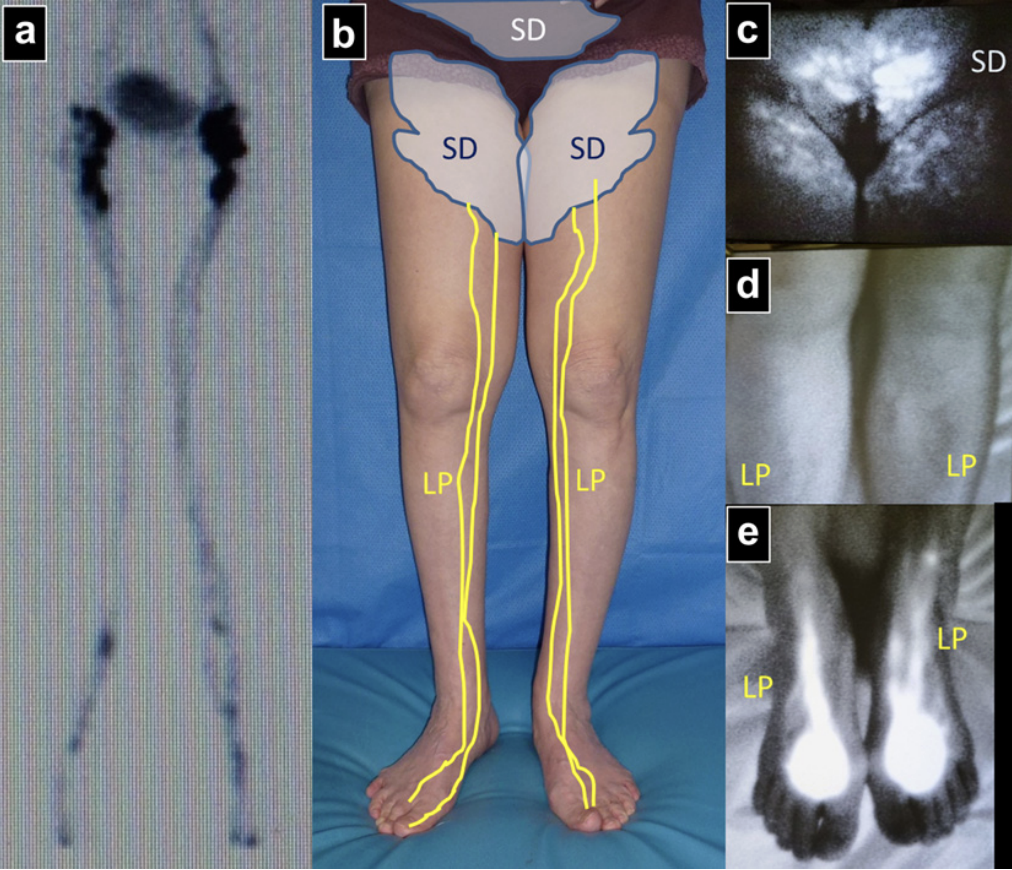
ICG Lymphography Patterns in Early Lymphatic Dysfunction
This image demonstrates the complementary roles of lymphoscintigraphy and indocyanine green (ICG) lymphography in assessing lymphatic function.
Despite normal lymphoscintigraphy (a) and no clinical asymmetry, ICG lymphography reveals early pathology: a stardust (SD) pattern in the proximal thighs and lower abdomen, alongside preserved linear patterns (LP) distally. This reflects early dermal backflow, where lymphatic overload leads to leakage into the dermis before overt vessel failure.
ICG lymphography is more sensitive than conventional imaging, detecting subclinical lymphatic dysfunction before measurable limb swelling develops. The transition from linear - splash - stardust - diffuse patterns represents progressive disease.
Technique Tip
Lymphaticovenous Anastomosis (LVA)
Lymphaticovenous anastomosis (LVA) is a supermicrosurgical procedure that diverts lymphatic fluid directly into the venous system by connecting functioning lymphatic channels to nearby venules. The operation is performed through small incisions using vessels that are often less than 0.8 mm in diameter, making it one of the most technically demanding procedures in reconstructive microsurgery.
This video follows patients from assessment through surgery, highlighting the importance of patient selection, lymphatic mapping, and meticulous supermicrosurgical technique. It provides an overview of how physiologic lymphatic reconstruction is performed and why LVA has become a key treatment option for lymphedema.
Building in Public
How I Operate: Releasing Soon!

Each episode follows the journey behind an idea. Starting from the problem, to the moment something had to change, to the trial and error that turned a technique into something teachable, repeatable, and useful.
Moving beyond what happens in theatre, we discuss judgment, progress, and the stories behind surgical innovation.
Watch out on Spotify for more snippets dropping soon!
What Does the Evidence Say?
Reverse Lymphatic Mapping in VLNT
The most useful takeaway is that this is not just anatomy. It matters clinically. In a prospective groin-VLNT series using reverse lymphatic mapping, no patient developed donor-site lymphedema, and lower-limb drainage was preserved in all cases. More recent prospective data also support donor-site safety: after groin VLNT with reverse mapping, no patient had a >10% lower-extremity volume difference at 12 months, and most donor-site adverse events were minor. Broader review-level evidence suggests that donor-site complication rates are generally low across VLNT donor sites.
However, reporting remains inconsistent, so reverse mapping is best understood as a risk-reduction strategy, not an absolute guarantee.
Sources: (Pons, 2021); (Pajula, 2024); (Dayan, 2015); (Raman, 2023)
Articles of the Week
3 Interesting Articles with One-Sentence Summaries
Indocyanine green (ICG) velocity offers a rapid, clinical way to assess lymphatic pump function, dropping predictably as lymphedema worsens, and unlike transit time (which can take over an hour in severe disease), ICG velocity can be measured in just 5 minutes.
Lymphedema after breast surgery is driven not just by lymphatic failure but also by increased capillary filtration and limb blood flow, creating a persistent fluid overload that surgeons must account for in management.
ICG lymphography shows a predictable progression from linear flow to splash, stardust, and diffuse dermal backflow, closely mirroring clinical stage and offering a quick, visual method to stage disease and guide timing and targeting of lymphatic surgery.
