
In this week's edition
- ✍️ Letter from P'Fella
What actually happens after you press submit? - 🖼️ Image of the Week
The 1984 description of the ALT Flap - 🚑 Technique Tip
Guide: Research methods in plastic surgery - 🎧 How I Operate
Not all muscle flaps behave the same - 📖 What Does the Evidence Say?
Could someone reproduce your study? - 🔥 Articles of the Week
Research in plastic surgery - 💕 Feedback
Suggest ideas & give feedback!
A Letter from P'Fella
What Actually Happens After You Press Submit?
From the outside, the editorial process can feel like a black box. One paper is rejected before it reaches peer review, while another gets sent out. Reviewer comments can point in completely different directions. A project you’ve spent months on can come back with a two-line decision, and you have no way of knowing whether the problem was the research, the writing, or simply that it wasn’t the right fit for the journal.
The strange thing is that we spend years learning how to write papers, but very little time understanding how they're actually read. We learn study design, statistics, and reporting guidelines, but almost nobody explains what an editor is looking for when a manuscript lands on their desk. What makes them keep reading? What makes them decide, within a few minutes, that a paper isn't the right fit? At what point does a reviewer become involved, and how much influence do they really have on the final decision? Those are the parts of research that most people only learn through trial and error.
Most of us spend our time trying to become better authors, but I've come to realize that understanding the perspective of an editor is probably just as valuable. It might not guarantee publication, but it might help you write a stronger paper before you even press submit.
That's why we’re planning a podcast recording with journal editors (we will soon reveal who they are!) to open that process up a little. I wouldn't want it to become a polite conversation about just impact factors and publication numbers. The goal is to ask the practical questions that need to be brought to light. We want to understand the decisions that happen before reviewer comments arrive, the common mistakes authors make, and the things that journals wish more researchers knew.
So, I’d like you to use this opportunity to ask the questions you actually care about when it comes to research. What would you ask the person on the other side of the process?
P’Fella ❤️
Image of the Week
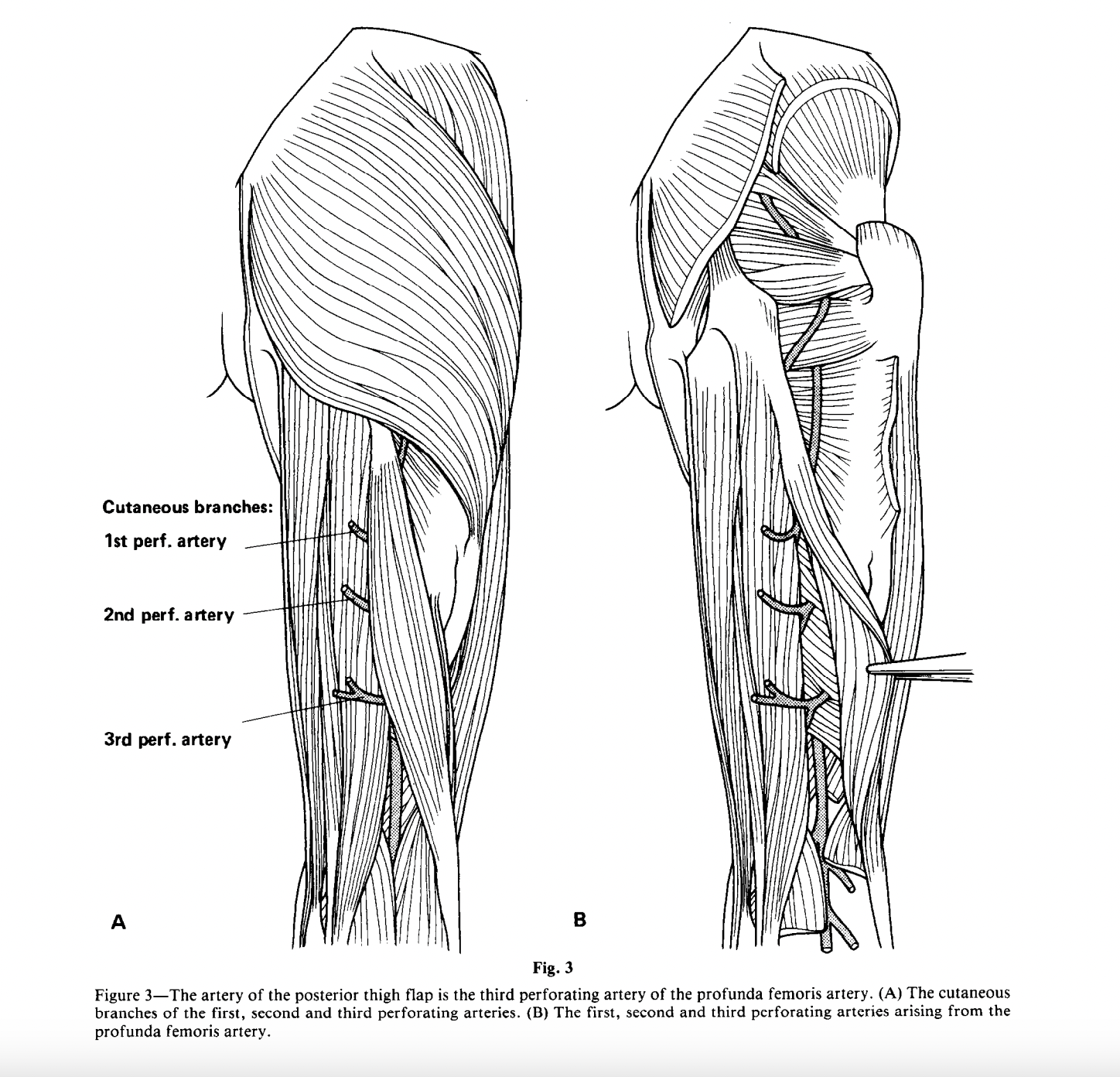
The 1984 Description of the Anterolateral Thigh (ALT) Flap
This week's image is from Song et al.’s original 1984 description of the anterolateral thigh (ALT) flap. At the time, this was a hypothesis that reliable skin flaps could be based on these perforators without sacrificing muscle.
What’s striking is how this single anatomical observation evolved into one of the most versatile flaps in modern microsurgery. Today, the ALT flap is used routinely for soft tissue reconstruction across the body.
Most impactful papers don’t begin with complex trials. They start with an observation, a clear anatomical insight, and the willingness to question existing dogma.
This is what publishing in plastic surgery often looks like at its best:
👉 See something others haven’t
👉 Define it clearly
👉 Show how it changes practice
Technique Tip
Research Methods in Plastic Surgery
Great research starts long before data collection. Choosing the right study design, understanding bias, selecting appropriate outcome measures, and critically appraising the literature are all essential skills for producing meaningful, publishable work.
This week's technique tip highlights our Research Methods in Plastic Surgery guide. This is a practical resource covering study designs, systematic reviews, patient-reported outcome measures (PROMs), qualitative research, and evidence appraisal.
How I Operate
Not All Muscle Flaps Behave the Same
Type V is where things get especially interesting: a major pedicle with secondary segmental pedicles, allowing the muscle to be turned over or rotated in different ways.
Rather than just memorising types, the classification was built to understand vascular anatomy well enough to make muscle flaps safer, more reliable, and more useful.
Prof. Foad Nahai on How I Operate
What Does the Evidence Say?
Could Someone Reproduce Your Study?
More recent evidence suggests that the problem persists. Among 727 original articles published in seven leading plastic surgery journals, only 1.5% included a data-sharing statement, and stated availability did not necessarily translate into data being provided when requested. Patient confidentiality and consent can limit what clinical researchers are able to share, but reproducibility does not always require publishing an identifiable dataset. A clear protocol, precise eligibility criteria, detailed outcome definitions, a complete statistical plan, and transparent reporting of any deviations can still allow readers to scrutinise and build on the work.
The practical lesson begins before submission. Authors should select the relevant reporting guideline, such as CONSORT, STROBE, PRISMA, or CARE while planning the study, rather than treating it as a final checklist. Where appropriate, protocols and analyses should be preregistered, and deidentified data, materials, and code should be shared when ethical and feasible.
The goal is not simply to get the paper accepted. It is to leave enough of a research trail that someone else could understand, test, and extend its findings.
(Ascha, 2019); (Ascha, 2022); (Keefer, 2025); (Douglas, 2014); (Becker, 2013)
Articles of the Week
3 Interesting Articles with One-Sentence Summaries
Plastic surgery RCTs frequently include patient-reported outcomes, but report less than 40% of CONSORT-PRO criteria, meaning patient perspectives are often captured but not clearly or reliably communicated for clinical use.
Half of surgeons in LMICs struggle to access journals, with paywalls, poor institutional access, and cost limiting both research output and the ability to stay clinically up to date.
Most research priorities are set in high-income settings with limited patient and multidisciplinary input, raising concerns that funded research may not reflect real clinical needs or global disease burden.
