
In this week's edition
- ✍️ Letter from P'Fella
What consistently shows up in skilled surgeons - 🎧 How I Operate
Episode one: Releasing tomorrow! - 🖼️ Image of the Week
Reconstruction determined by the defect - 🚑 Technique Tip
SCIP flap harvest - 🎓 Building in Public
Catching up with the team - 📖 What Does the Evidence Say?
Venous congestion in free flaps - 🔥 Articles of the Week
Supermicrosurgery in lower limb, predict free flap failure, & MSAP flap - 💕 Feedback
Suggest ideas & give feedback!
A Letter from P'Fella
What Consistently Shows Up in Skilled Surgeons
They reply to emails quickly. And at some point in their training, they’ve usually had proper cadaver exposure. That's it.
The first one sounds small, but it tells you a lot. People who are organised, switched on, and serious about their work tend to move quickly. It’s not about trying to impress anyone. It usually comes from simple habits around being reliable. The second one feels even more important. Again and again, when I speak to surgeons whose understanding feels really deep, not just technically good but properly three-dimensional, cadaver work is somewhere in the background.
That makes sense, really. There are some things you can’t learn properly from slides, or diagrams, or even theatre alone. Cadaver labs give you time. Time to slow down. Time to see where things actually sit. Time to make mistakes without consequence. Time to understand anatomy with your hands, not just your eyes. And the more I think about it, the more I feel this is one of the areas we’re starting to lose.
Access to cadaver labs feels harder now than it should be. Costs, rules, legislation, and logistics all play a part, and what should be a core part of surgical training can end up feeling rare or out of reach. That’s a shame, and it’s something we shouldn’t just accept. If we’re serious about training people well, then we should be trying to bring that access back, not letting it slowly disappear.
We talk about this a bit in some of the upcoming podcast episodes as well. A few of the people I’ve spoken to make this point in their own way, and it’s interesting how often it comes back to the same thing: the best surgeons usually didn’t just read anatomy. They spent time with it.
And on that note, the podcast drops tomorrow. We’ve spoken to some really interesting and influential people in plastics, and we’re super excited for you to check it out. Check it out on your preferred platform!
P’Fella ❤️
How I Operate
Episode One: Releasing Tomorrow!
Episode One Trailer: Releasing Tomorrow!
- Lymph node transfer: Especially for upper limb lymphoedema
- Ultra-thin reconstruction: Ideal for the dorsum of the hand or foot
- Facial contouring: Useful when submental or supraclavicular options are unavailable
Image of the Week
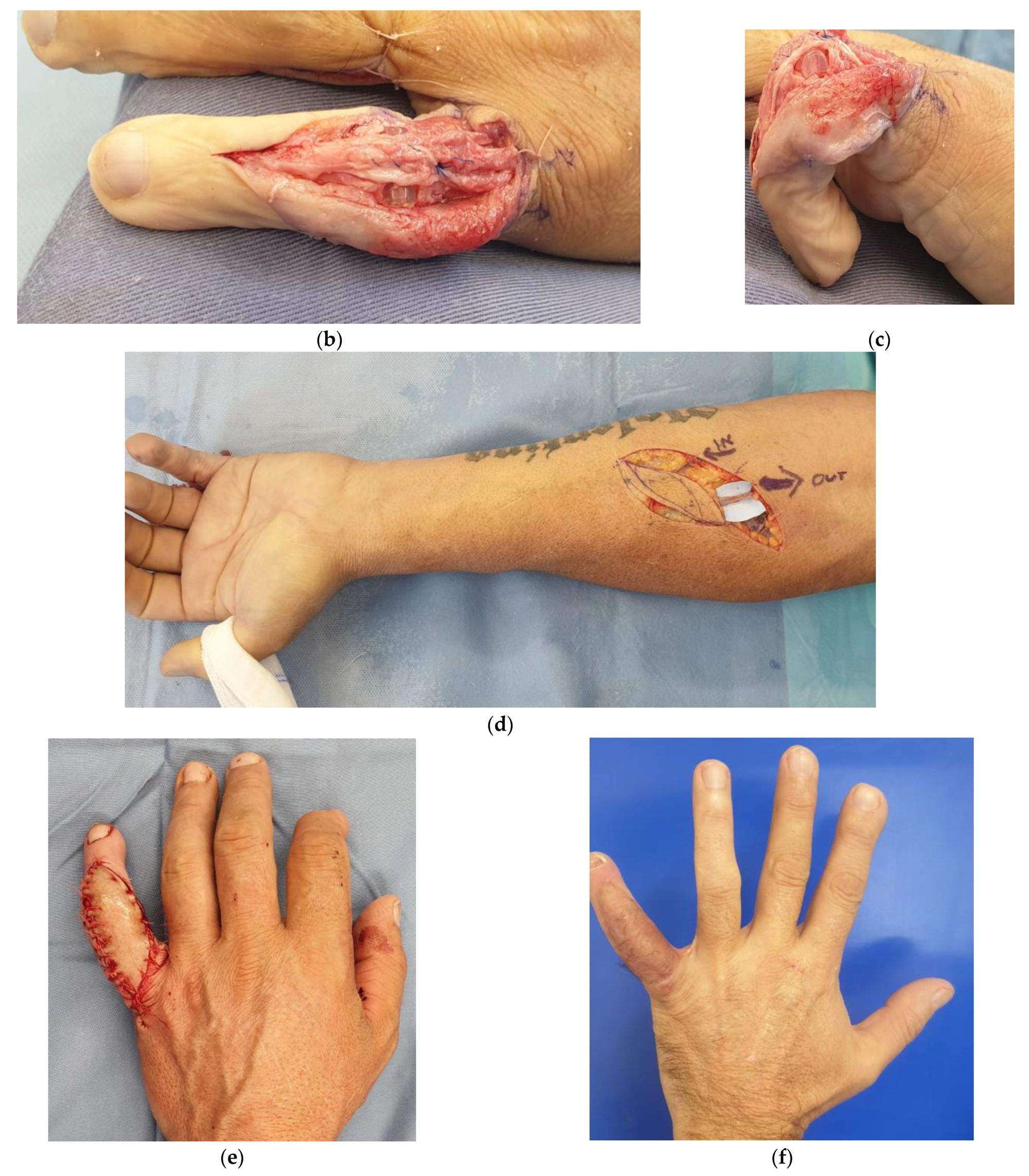
Reconstruction Determined by the Defect
The reconstruction is determined by the defect, not the other way around.
We see a traumatic thumb defect with exposed structures, followed by preoperative flap design on the forearm, elevation of a fasciocutaneous flap, inset, and final functional outcome. The key step isn’t the anastomosis, it’s the planning: selecting tissue with the right thickness, vascularity, and arc of rotation to restore both contour and function.
This reflects a shift in modern microsurgery, moving beyond “can we do a free flap?” to “what is the best reconstructive option for this specific defect?”
The end result demonstrates what good planning achieves: in addition to survival of the flap, durable coverage, preserved length, and functional recovery.
Technique Tip
SCIP Flap Harvest
The SCIP (Superficial Circumflex Iliac Artery Perforator) flap is a versatile, thin perforator flap with minimal donor-site morbidity.
This cadaveric demonstration highlights the key anatomical landmarks, identification of the medial and lateral perforators, and elevation of the flap in the superficial fascial plane.
A valuable insight from the video is to identify the perforators before committing to pedicle dissection. Assessing perforator size, course, and venous drainage early allows the surgeon to select the most suitable pedicle and tailor the flap to the reconstructive requirements.
Professor JP Hong will be the first guest on our new "How I Operate" podcast series. Join us as we discuss the evolution of the SCIP flap, including flap design, perforator selection, harvest techniques, and the principles.
Subscribe and stay tuned!
Building in Public
Catching Up with the Team
Different countries, different training systems, different perspectives, but the same shared goal: to build the best possible educational product for plastic surgery.
What Does the Evidence Say?
Venous Congestion in Free Flaps
The evidence also suggests that prevention is more reliable than rescue. In pooled analyses, double venous anastomosis has been associated with lower flap failure and fewer venous complications overall, although this benefit is not uniform across every setting and appears less clear in lower-limb reconstruction specifically. Once venous congestion occurs, the best-supported first step remains surgical revision to restore mechanical outflow. Beyond that, the evidence for adjuncts is much weaker: systematic review data suggest that, of the nonsurgical options, medicinal leeches have the strongest clinical support, whereas other measures remain supported mainly by low-level evidence.
The practical takeaway is simple. Build reliable venous drainage at the index operation, and treat postoperative congestion as a time-critical surgical problem.
Sources: (Riot, 2015); (Boissiere, 2021); (Weinzweig, 1995); (Matthews, 2017); (Kubo, 2002)
Articles of the Week
3 Interesting Articles with One-Sentence Summaries
Perforator-to-perforator supermicrosurgery is a safe and efficient option for lower extremity reconstruction, offering high flap survival with less vessel morbidity but requiring advanced technical skill.
Developing a practical risk index showing that comorbidities and defect etiology strongly predict vascular compromise and flap failure, to help surgeons stratify risk & guide reconstructive decision-making.
The MSAP flap offers a thin, low-morbidity alternative to RFFF but carries a higher risk of late venous thrombosis, making vigilant monitoring and dual venous anastomoses critical for flap survival.
