
In this week's edition
- ✍️ Letter from P'Fella
Why are doctors leaving their careers so early? - 🖼️ Image of the Week
Fascial architecture of the inframammary fold - 🚑 Technique Tip
Superior pedicle breast reduction - 🎓 Building in Public
Updates from the On-Call Team - 📖 What Does the Evidence Say?
Blood supply to the nipple - 🔥 Articles of the Week
Aesthetic breast dimensions, patient-reported outcome measure for breast surgery, & 5 Decisions in breast augmentation. - 💕 Feedback
Suggest ideas & give feedback!
A Letter from P'Fella
Why Are Doctors Leaving Their Careers So Early?
Late 40s is not the end of a medical career. Not after that much training, that much sunk time, and that much personal cost.
So what were the reasons? Hassle factor, stress, unrealistic patient demands, and lack of professional satisfaction were the biggest ones. Overwork and frustration with health-system structures kept coming up too. None of that reads like a motivation problem. It reads like people getting worn down by the shape of the job itself.
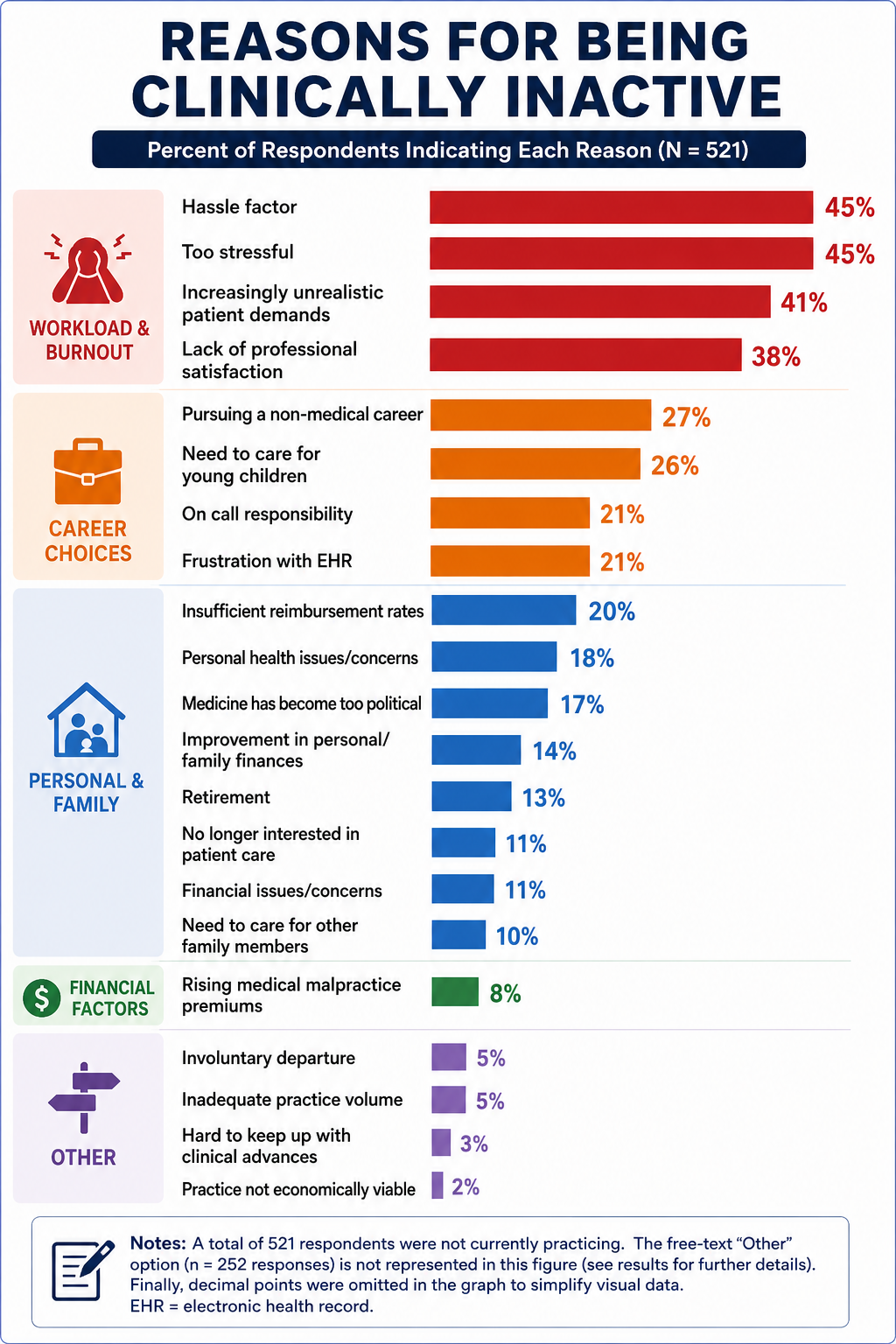
The gender side of it is hard to ignore as well. Women made up 63.9% of respondents, were more likely than men to say they left to care for children or other family members, and among doctors no longer practicing, the median clinical career was 9 years for women versus 12 for men.
We talk about workforce shortages as if the answer is mostly at the front end: train more people, open more posts, widen the pipeline. But if fully trained doctors are leaving in their 40s, and some never enter practice at all, then the problem sits much further downstream too. You can’t keep talking about recruitment while ignoring what clinical work has become for the people already inside it.
If we want doctors to stay, the job has to feel worth staying in. That means less pointless friction, less admin disguised as care, better support for family life, and a lot more of looking into why good people are walking away, so we can fix the issues from within. Otherwise, we’ll keep calling it a workforce problem when really it’s a retention problem we’ve been watching in plain sight.
P’Fella ❤️
Image of the Week
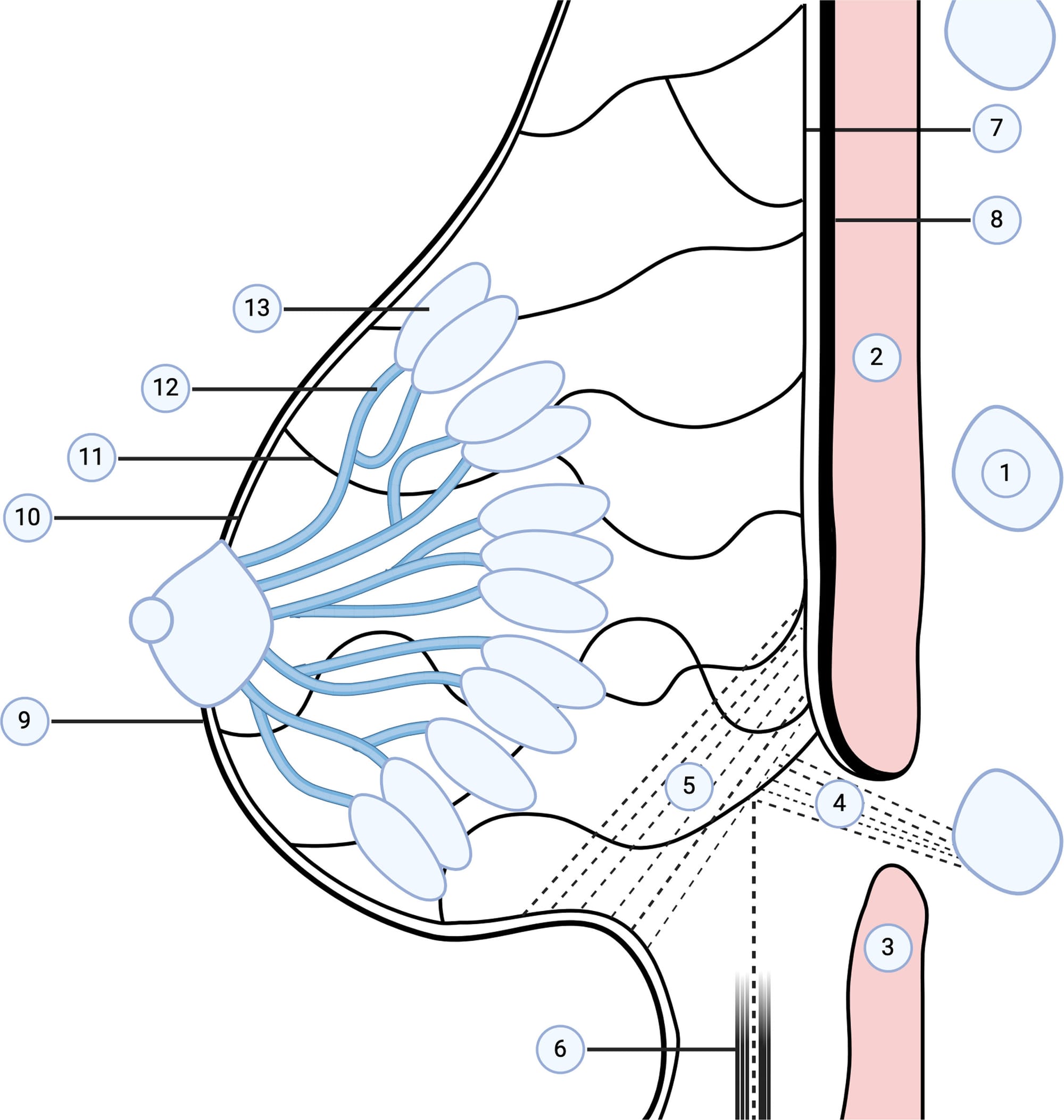
Fascial Architecture of the Inframammary Fold
This schematic highlights the inframammary fold (IMF): a key structure defining the lower pole contour and breast footprint.
The IMF is not a single ligament, but a fascial system formed by:
- (1) Breast parenchyma
- (2) Skin envelope
- (4-5) Superficial and deep fascial layers
- (6) Chest wall
- (9-13) Fibrous septa extending from the dermis to deep fascia
These septa create a zone of adherence, anchoring the breast and defining the fold.
Clinically:
- It is critical for implant positioning and symmetry
- Disruption leads to double-bubble deformity or bottoming out
- Breast aesthetics depend on restoring this fascial architecture, not just skin or volume.
Technique Tip
Superior Pedicle Breast Reduction
The superior pedicle technique preserves vascularity to the nipple-areola complex through a superiorly based dermoglandular pedicle while allowing resection of excess inferior and lateral breast tissue. It is particularly useful for mild to moderate reductions where significant nipple transposition is not required.
A key technical point is maintaining adequate pedicle thickness to preserve blood supply while achieving sufficient parenchymal resection for breast shaping. The technique also facilitates upper pole fullness and reliable nipple positioning, making it a versatile option for both functional and aesthetic breast reduction surgery.
Building in Public
Updates from The On-Call Team
A major theme of the discussion was strengthening quality control, with the team agreeing on refining the current structured approach to article development, with clearer learning objectives, stronger reviewer feedback, and a continued emphasis on accuracy and usability 🚀
What Does the Evidence Say?
Blood Supply to the Nipple
The clinical evidence from nipple-sparing mastectomy reinforces the same principle. Once breast tissue is undermined or retroareolar tissue is separated, nipple viability depends less on a single named artery and more on preservation of the dermal-subdermal plexus, flap thickness, incision choice, and patient factors. Thin flaps, circumareolar scars, smoking, previous radiotherapy, large or ptotic breasts, and aggressive undermining all increase concern for ischaemia. Delay procedures work for the same reason: they precondition collateral flow before definitive surgery.
The most evidence-based takeaway is therefore that the nipple has a rich but vulnerable collateral blood supply. In practice, preserving the dermal/subdermal plexus and an adequately thick, well-perfused pedicle is most important.
Sources: (Nimboriboonporn, 2014); (Del Riego, 2020); (Lohsiriwat, 2012); (Jensen, 2012); (Chirappapha, 2014); (Lee, 2023)
Articles of the Week
3 Interesting Articles with One-Sentence Summaries
Defining four objective parameters of the “ideal” breast - 45:55 upper-to-lower pole ratio, upward nipple angulation, straight/concave upper pole, and convex lower pole, to guide aesthetic surgical planning.
A multicentre study developing and validating the BREAST-Q, a reliable patient-reported outcome tool assessing satisfaction and quality of life across six domains in breast surgery patients.
A structured, measurement-based “High Five” planning system can streamline breast augmentation decision-making while achieving very low reoperation rates (~3%).
